CARDIOVASCULAR JOURNAL OF AFRICA • Vol 23, No 1, February 2012
e20
AFRICA
CARDIOVASCULAR JOURNAL F AFRICA • Vol 22, No 5, September/October
1
276
disk. Also, there are small foam segments in the middle to ‘plug’
the tunnel of the PFO (which may sometimes be widened by the
passage of the delivery sheaths). The device is fully retrievable
before release and makes use of a special bioptome, which can
be locked to prevent accidental release. All sizes are delivered
using 9F–12F long sheaths.
Both patients presented with ASA and multi-fenestrated
PFOs. We determined it might be feasible to close the PFO with
a single device that would also cover the other smaller more
posterior defects. Initial inspection of the interatrial septum
suggested that the PFOs were small but the ASAs were large. The
options of surgical resection of the ASA and defect closure were
offered for the patients’ consideration. Both opted for attempted
device closure first.
We selected a 30-mm Atriasept™ II PFO occluder with large
retention disks, which would be sufficient to cover all the defects
and stabilise the ASA. With proper positioning on the interatrial
septum, we ensured that the left and right disks of the device
covered most defects and did not impinge on the mitral valve.
Thus, with advanced consideration and planning, we were able
to successfully close multiple defects with a single Atriasept II
device.
In addition to the economic benefit of using only one
device instead of multiple devices, we believe this approach
offers several advantages including less implanted material, less
manipulation and insult to internal cardiac tissues, as well as
shorter procedure times. The results were both immediate and
complete with no residual shunting and a well-contained ASA.
Although not all defects were covered by the device, stabilisa-
tion of the ASA seemed to result in spontaneous closure of some
defects.
On a practical note, the operators found the fact that the
central portion of the device can be elongated by pushing the
device out, up to the proximal limbs of the right atrial disk made
it easier to accurately position the device, especially in long PFO
tunnels (Fig. 4). It also allows some compensation for the offset
between the left and right atrial disks in these longer tunnels.
It is important to realise that not all PFOs with fenestrated
ASAs qualify for transcatheter device closure. Our patients were
essentially considered because of a history of recurrent strokes
in the presence of a PFO. Furthermore, both major complications
(
<
1%) such as pericardial tamponade and infection, as well as
minor complications (6%) such as bleeding, thrombus forma-
tion, etc have been described with virtually all the PFO devices
in use.
17-20
Conclusion
In both cases we were successful in closing multiple defects and
stabilising the ASA with a single device, providing enhanced
economic benefit and clinical outcome. Our limited experi-
ence suggests that the Atriasept™ II PFO occluder is a safe and
effective device for patients with multiple defects and associated
ASAs.
References
1. Hagen PT, Scholz DG, Edwards WD. Incidence and size of patent fora-
men ovale during the first 10 decades of life: an autopsy study of 965
normal hearts.
Mayo Clin Proc
1984;
59
: 17–20.
2. Overell JR, Bone I, Lees KR. Interatrial septal abnormalities and
stroke – a meta-analysis of case-control studies.
Neurology
2000;
55
:
1172–1179.
3. Negrão EM, Brandi IV, Nunes SV,
et al
. Patent foramen ovale and
ischemic stroke in young people: statistical association or causal rela-
tion?
Arq Bras Cardiol
2007;
88
: 514–520.
4. Mas JL, Arquizan C, Lamy C,
et al
. Recurrent cerebrovascular events
associated with patent foramen ovale, atrial septal aneurysm or both.
N
Engl J Med
2001;
345
: 1740–1746.
5. Leurmans JGLM, Post HWM, ten Berg JM,
et al.
Complications and
mid-term outcome after percutaneous patent foramen ovale closure in
patients with cryptogenic stroke.
Neth Heart J
2008;
16
: 332–336.
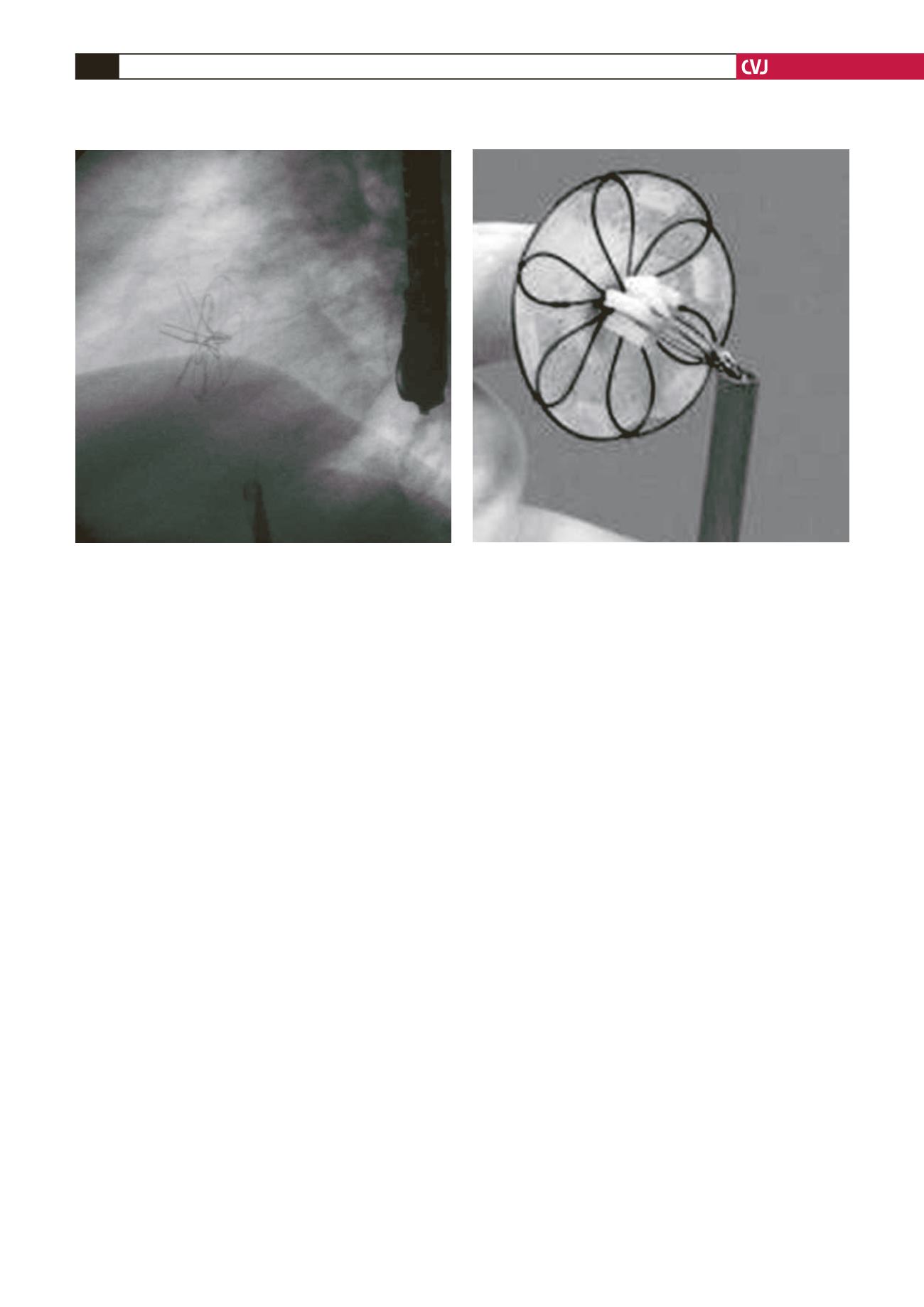
Fig. 4. Atriasept device. The foam in the central aspect
of the device can be seen. The left atrial disk can be
seen and the proximal limbs of the right disk have been
pushed out from the long sheath. See text for further
details.
Fig. 3. Lateral radiographic view of device after release.
disk. Also, there re small foam segme ts in the middle to ‘plug’
the unnel of the PFO (which may s metimes be widened by he
passage of the delivery sh aths). Th device is fully r trievabl
before release and makes use of a special bioptome, which can
be locked to prevent accidental release. All sizes are delivered
using 9F–12F long sheaths.
Both patients presented with ASA a d multi-fenest ated
PFOs. We determi ed it might be feasible to c ose the PFO with
a single device that would also cover the other smaller more
manipul
shorter
complet
Althoug
tion of t
defects.
On a
central p
device o
it easier t
tunnels (
between
It is i
ASAs q
essential
in the pr
(
<
1%) s
minor c
tion, etc
in use.
17-2
Concl
In both c
stabilisin
economi
ence sug
effective
ASAs.
Refere
1. Hage
men
norm
2. Over
strok
1172
3. Negr
ische
tion?
4. Mas
assoc
Engl
5. Leur
mid-t
patie
Fig. 4. Atriasept device. The foam in the central aspect
of the device can be seen. The left atrial disk can be
seen and the proximal limbs of the right disk have been
push d ut f om the long sheath. See text for further
details.
Fig. 3. Lateral radiographic view of device after release.
disk. Also, there are small foam segments in the middle to ‘plug’
the tunnel of the PFO (which may sometimes be widened by the
passage of the delivery sheaths). The device is fully retrievable
before release and makes use of a special bioptome, which can
be locked to prevent accidental release. All sizes are delivered
using 9F–12F long sheaths.
Both patients presented with ASA and multi-fenestrated
PFOs. We determined it might be feasible to close the PFO with
a single device that would also cover the other smaller more
complete with no residual shunting and a well-contained ASA.
Although not all defects were covered by the device, stabilisa-
tion of the ASA seemed to result in spontaneous closure of some
defects.
On a practical note, the operators found the fact that the
central portion of the device can be elongated by pushing the
device out, up to the proximal limbs of the right atrial disk made
it easier to accurately position the device, especially in long PFO
tunn ls (Fig. 4). It also lows some c mpensation for the offset
betw en the left and right atrial disks in these long tunn ls.
It i impo tant to r alise that not all PFOs wi h fenestrated
ASAs qualify for tra catheter dev ce closure. Our patients were
essential y cons dered because of a history of recurrent strokes
in the pr sence of a PFO. Fu thermore, both major complications
(
<
1%) such as pericardia tamponade and infection, as w ll a
minor complications (6%) such as bleedi g, thrombus form -
tion, etc hav been described wi h virtually all the PFO devices
in use.
17-20
Conclusion
In both cases we were successful in closing multiple defects and
stabilising the ASA with a single device, providing enhanced
economic benefit and clinical outcome. Our limited experi-
ence suggests that the Atriasept™ II PFO occluder is a safe and
effective device for patients with multiple defects and associated
ASAs.
References
1. Hagen PT, Scholz DG, Edwards WD. Incidence and size of patent fora-
men ovale during the first 10 decades of life: an autopsy study of 965
normal hearts.
Mayo Clin Proc
1984;
59
: 17–20.
2. Overell JR, Bone I, Lees KR. Interatrial septal abnormalities and
stroke – a meta-analysis of case-control studies.
Neurology
2000;
55
:
1172–1179.
3. Negrão EM, Brandi IV, Nunes SV,
et al
. Patent foramen ovale and
ischemic st oke in young peop e: statistical association or causal rela-
tio ?
Arq Br s Cardiol
2007;
88
: 514–520.
4. Mas JL, Arquizan C, Lamy C,
et al
. Recurrent cerebrovascular events
associated with patent foramen ovale, atrial septal aneurysm or both.
N
Engl J Med
2001;
345
: 1740–1746.
5. Leurmans JGLM, Post HWM, ten Berg JM,
et al.
Complications and
mid-term outcome after percutaneous patent foramen ovale closure in
patients with cryptogenic stroke.
Neth Heart J
2008;
16
: 332–336.
Fig. 4. Atriasept device. The foam in the central aspect
of the device can be seen. The left atrial disk can be
seen and the proximal limbs of the right disk have been
pushed out from the long sheath. See text for further
details.
Fig. 3. Lateral radiographic view of device after release.
CARDIOVASCULAR JOURNAL OF AFRICA • Vol 22, N 5, September/O tober 2011
276
AFRICA
disk. Also, there are small foam segments in the middle to ‘plug’
the tunnel of the PFO (which may sometimes be widened by the
passage of the delivery sheaths). The device is fully retrievable
before release and makes use of a special bioptome, which can
be locked to prevent accidental release. All sizes are delivered
using 9F–12F long sheaths.
Both patients presented with ASA and multi-fenestrated
PFOs. We determined it might be feasible to close the PFO with
a single device that would also cover the other smaller more
posterior defects. Initial inspection of the interatrial septum
suggested that the PFOs were small but the ASAs were large. The
options of surgical resection of the ASA and defect closure were
offered for the patients’ consideration. Both opted for attempted
device closure first.
We selected a 30-mm Atriasept™ II PFO occluder with large
retention disks, which would be sufficient to cover all the defects
and stabilise the ASA. With proper positioning on the interatrial
septum, we ensured that the left and right disks of the device
covered most defects and did not impinge on the mitral valve.
Thus, with advanced consideration and planning, we were able
to successfully close m ltiple defects with a singl Atriasept II
device.
I additio to the economic benefit of using only one
device instead of multiple devices, we believe this appro ch
o rs s veral advant ges including less implanted material, less
manipulation and insult to internal cardiac tissues, as well as
shorter procedure times. The results were both immediate and
complete with no residual shunting and a well-contained ASA.
Although not all defects were covered by the device, stabilisa-
tion of the ASA seem d to result in spontaneous closure of some
defects.
On a practical note, the operators found the fact that the
central portion f the device can be elongated by pushing the
device out, up to the proximal limbs of the right atrial disk made
it easier to accurately position the device, especially in long PFO
tunnels (Fig. 4). It also allows some compensation for the offset
between the left and right atrial disks in these longer tunnels.
It i important to realise that not all PFOs with fenestrated
ASAs qualify for transcatheter device closure. Our patients were
essentially considered because of a history of recurrent strokes
in the presence of a PFO. Furthermore, both major complications
(
<
1%) such as pericardial tamponade and infection, as well as
minor complications (6%) such as bleeding, thrombus forma-
tion, etc have been described with virtually all the PFO devices
in use.
17-20
Conclusion
In both cases we were successful in closing multiple defects and
stabilising the ASA with a single device, providing enhanced
economic benefit and clinical outcome. Our limited experi-
ence suggests that the Atriasept™ II PFO occluder is a safe and
effective device for patients with multiple defects and associated
ASAs.
References
1. Hagen PT, Scholz DG, Edwards WD. Incidence and size of patent fora-
men ovale during the first 10 decades of life: an utopsy study of 965
normal hearts.
M yo Clin Proc
1984;
59
: 17–20
2. Overell JR, Bone I, Lees KR. Interatrial septal abnormalities and
stroke – a meta- alysis of ca e-control studies.
Neu ology
2000;
55
:
1172–1179.
3. Negrão EM, Br n IV, Nunes SV,
et al
Patent foramen ovale and
ischemic stroke i young peopl : statisti al association or ausal r la-
tion?
Arq Bras C rdiol
2007;
88
: 514–520.
4. Mas L, Arquizan C, Lamy C,
et al
. Recurrent cerebrovascular events
associated with patent foramen ovale, atrial sep al aneurysm or both.
N
Engl J Med
2001;
345
: 1740–1746.
5. Leurmans JGLM, Post HWM, ten Berg JM,
et al.
Complications and
mid-term outcome after percutaneous patent foramen ovale closure in
patients with cryptogenic stroke.
Neth Heart J
2008;
16
: 332–336.
Fig. 4. Atriasept device. The foam in the central aspect
of the device can be seen. The left atrial disk can be
seen and the proximal limbs of the right disk have been
pushed out from the long sheath. See text for further
details.
Fig. 3. Lateral radiographic view of device after release.
FRICA • Vol 22, No 5, September/October 2011
AFRICA
posterior defects. Initial inspection of the interatrial septum
suggested that the PFOs were small but the ASAs were large. The
options of surgical resection of the ASA and defect closure were
offered for the patients’ consideration. Both opted for attempted
device closure first.
We selected a 30-mm Atriasept™ II PFO occluder with large
retention disks, which would be sufficient to cover all the defects
and stabilise the ASA. With proper positioning on the interatrial
septum, we ensured that the left and right disks of the device
covered most defects and did not impinge on the mitral valve.
Thus, with advanced consideration and planning, we were able
to successfully close multiple defects with a single Atriasept II
device.
In addition to the economic benefit of using only one
device instead of multiple devices, we believe this approach
fers sev ral adv ntages including l ss implanted materi l, less
manipulation and insult to internal cardiac tissues, s well as
shorter procedure times. The re ults were both imm diate and
complet with no residual s unting and a well-contai
ASA.
Although not all defect were cover d by the device, stabilisa-
tion of the ASA see ed to result in ontane us closure of some
d fects.
On a practical note, the operators found the fact that the
central portio of th device can be elongated by pushing he
device out, up to th proximal limbs of th right atrial disk made
it easier to ac urately p sition the de ice, especially in ong PFO
tunnels (Fig. 4). It also allows some compensation for the offset
between the left and right atrial disks in these longer tunnels.
It is important to realise that not all PFOs with fenestrated
ASAs qualify for transcatheter device closure. Our patients were
lease.


