CARDIOVASCULAR JOURNAL OF AFRICA • Vol 22, No 6, November/December 2011
AFRICA
327
EPA to DHA ratio
Fish oils from different sources contain variable mixtures of
EPA and DHA. Most commercially available fish oils contain
a proportion of 2:1 EPA to DHA.
22
Regarding the EPA to DHA
ratio in South African n-3 fatty acid supplements, most of the
studied supplements (40%;
n
=
18) had an EPA:DHA ratio of
1.51–2.0:1, while 36% (
n
=
16) of supplements had a 2.1–2.5:1
EPA:DHA ratio. Only a few (13%;
n
=
6) supplements had a
higher DHA:EPA ratio (EPA:DHA ratio
<
0.5) (see Table 1).
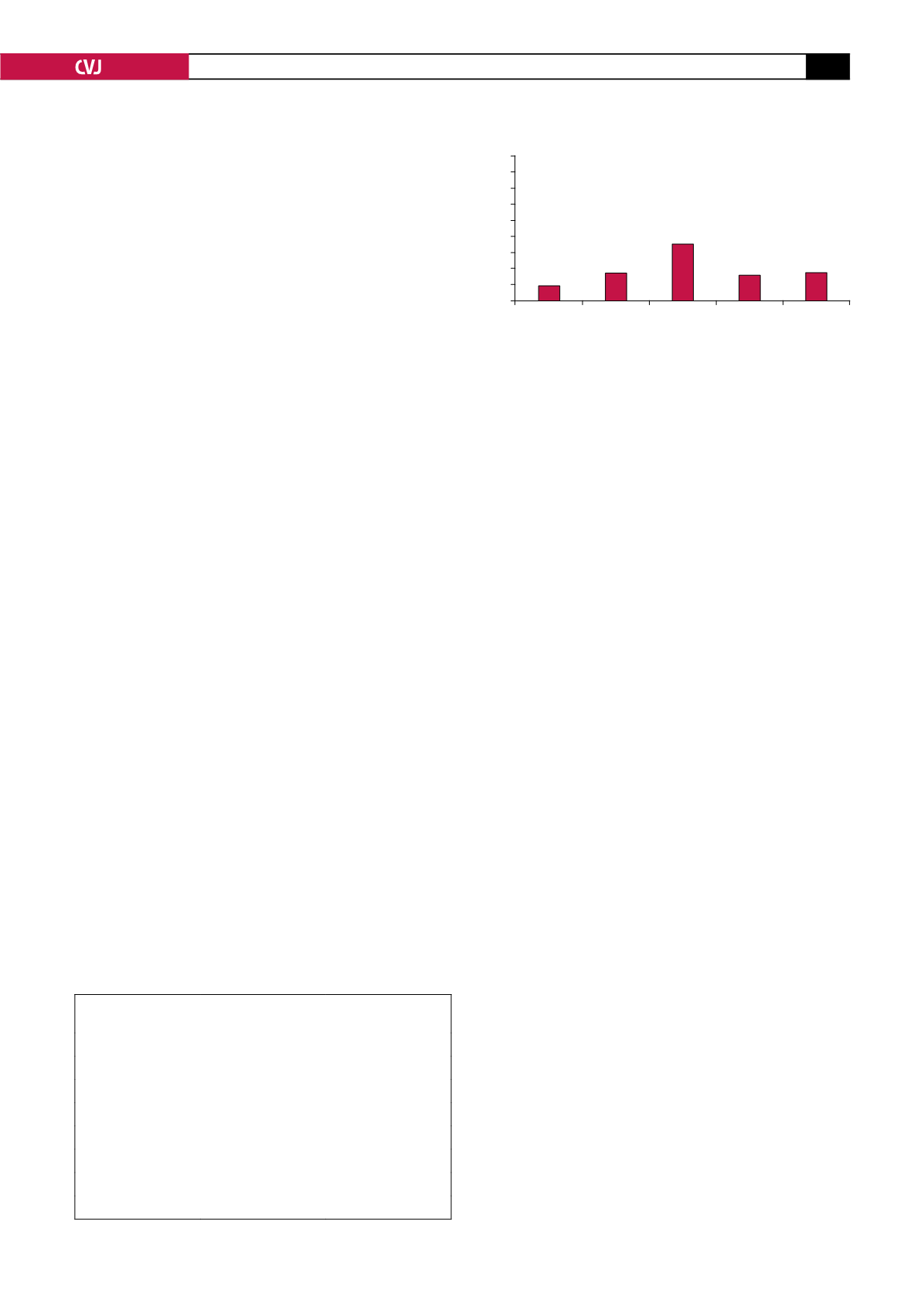
Conjugated dienes
The majority (73%;
n
=
33) of commercially available n-3 fatty
acid supplements had a CD content higher than 21
μ
M. Only
27% (
n
=
12) of the n-3 fatty acid preparations contained a CD
content of less than 20
μ
M, while barely any supplements (
n
=
4; 9%) contained a CD content comparable to fresh, unopened
oils (see Fig. 4). These values were measured notwithstanding
the presence of added vitamin E as an antioxidant.
Mercury contamination
Mercury was virtually absent from the oils in the supplements
and was therefore not of any health concern in these samples.
Discussion
An extensive variety of n-3 fatty acid supplements are available
to the South African consumer, however, our results have shown
that supplements vary to a large extent in terms of claimed and
measured EPA and/or DHA content, levels of fatty acid oxida-
tion, EPA to DHA ratio, as well as numbers of capsules and price
to meet international dietary recommendations. When comparing
claimed to measured contents of EPA and DHA in South African
n-3 fatty acid supplements, it is of concern that information
appearing on almost two-thirds of these supplements’ labels was
not a true reflection of the actual contents of the supplements. It
was decided to compare supplements against an arbitrary 90 to
110% standard. In other words, supplements’ label information
was considered as a truthful reflection of the measured content if
the EPA and/or DHA content analyses were between 10% less or
10% more, compared to the claimed content.
More than half of commercially available South African
n-3 fatty acid supplements failed to attain 90% of the claimed
contents of EPA or DHA or both, while approximately 15% of
supplements contained more than 110% of the claimed contents
of EPA or DHA or both. Since the typical Western diet is
characterised by a low n-3 and very high n-6 fatty acid intake,
many consumers rely on supplements to increase their daily n-3
intakes. Unfortunately, if unreliable information is published on
labels, consumers are supplied with misleading information,
leading to erroneous dosages, with subsequent consequences.
If a supplement contains less n-3 fatty acids than claimed,
consumers waste their money without optimal improvement
of their n-3 fatty acid status. In contrast, excess n-3 fatty acid
intakes can be just as detrimental as a deficiency. Adverse effects
of excess intake of n-3 fatty acids in healthy populations include
suppression of the immune function, bleeding and increased risk
of haemorrhagic stroke, as well as increased lipid peroxidation,
resulting in oxidative damage to various tissues. Furthermore,
simultaneous intake of n-3 fatty acids with medication such as
aspirin and warfarin will excessively prolong bleeding times
in individuals using anti-coagulants.
5
The FDA has ruled that
intakes of up to 3 g/d of marine n-3 fatty acids are generally
recognised as safe (GRAS) for inclusion in the diet.
5
Regarding the number of capsules needed to meet optimal
n-3 fatty acid intakes, our results indicate that only a few supple-
ments were able to provide the daily need in one capsule. Some
supplements even required a dosage of more than five capsules
to meet international recommendations. In addition to this, our
analyses have shown that the majority of n-3 supplements on the
South African market were priced between R2.01 and R5.00 per
day to meet the ISSFAL recommendation of 500 mg EPA
+
DHA
per day. This represents an amount of R60.30 to R150.00 per
individual per month. To provide a family of four with the daily
recommended intake of 500 mg EPA
+
DHA adds up to between
R242.40 and R600.00 per family per month.
Since malnutrition, especially in poverty-stricken areas, is a
major health problem in South Africa, it can be accepted that
many people have either a marginal or deficient n-3 fatty acid
status. Considering the current financial situation in South
Africa, in combination with a large part of the South African
population living in poverty, this amount is substantial in terms
of monthly expenses for the average South African family.
Hence, it is impossible for the average South African to consume
an n-3 fatty acid supplement on a regular basis. Some supple-
ments are even more expensive and can cost up to R1 060 per
person per month to meet the recommended intake of 500 mg
EPA
+
DHA per day.
The ratio of EPA to DHA in n-3 supplements has become
an important point of discussion. Gorjão
et al.
22
reported that
most commercially available fish oils present with a 2:1 ratio
of EPA to DHA, while numerous cold-water oily fish sources
TABLE 1. EPA TO DHA RATIO IN SOUTHAFRICAN N-3
FATTYACID SUPPLEMENTS
Ranges
EPA:DHA ratio (
n
)
EPA:DHA ratio (%)
<
0.5:1
6
13
– 1.5:1
2
4
1.51–2.0:1
18
40
2.1–2.5:1
16
36
2.51–3.0:1
0
0
3.0–3.5:1
1
2
>
5:1
2
4
Fig. 4. Conjugated diene content of South African n-3
fatty acid supplements.
45
40
35
30
25
20
15
10
5
0
Supplements (
n
=
5)
<
10
11–20
21–30
31–40
>
41
Conjugated dienes (
µ
M)
9%
18%
16%
39%
18%


