CARDIOVASCULAR JOURNAL OF AFRICA • Vol 23, No 3, April 2012
AFRICA
129
gap takes into account variable pericardial thicknesses, and
moreover, can be locked once a predetermined compressive
force has been applied to close the gap in which the pericardium
is located.
The grooved outer surface of the receptacle has a series of
rings that restrain the suture that binds the sewing ring material to
the receptacle (see Fig. 1). This material is rolled into a standard-
shaped sewing ring for passage of the surgical sutures used to
anchor the valve. The flared areas of the receptacle receive the
locking mechanism of the upper and lower frames, which engage
in a double-clip system at each of the three post regions.
The assembly of the valve components, as well as the
integration of the pericardial tissue into the frame was undertaken
to prove the viability of the concept. The frame components used
in this experiment were manufactured from a polymer certified
for surgical assistance and suitable for human tissue contact.
The assembled pericardial and frame components are shown in
Fig. 3.
Chrome cobalt sintering was used for the first time in recorded
heart valve literature to manufacture valve stents. Used currently
for dental applications, the sintering approach provided an
intricately manufactured product, with accurate reproducibility
from biostable material at an attractive cost and production time.
The leaflet material protruding through the posts combined to
form a tissue thickness of between 0.55 and 0.70 mm. The post,
containing a gap of 0.90 mm, allowed for ease of protrusion of
this fold of tissue. In order to secure the pericardium in place, a
surgical hemaclip, made from approved stainless steel grade 5, is
accurately applied after the pericardium has been pulled through
the gap. The hemaclip, together with the tissue, form a composite
section wider than the post-gap opening, preventing it from
pulling though the gap in the posts. The integrity of the hemaclip
also supports the vertical aspect of the pericardium, ensuring that
it does not fold and collapse under gravity.
Conclusion
As the world population fast approaches seven billion and the
growth rate of developing nations leads the way, the instances of
heart valve disease become more prevalent. Currently, the market
supplies heart valve replacements largely to those older than 65
years of age and who reside in developed parts of the world. A
vast portion of the market is limited by low income and poor
access to medical facilities. Lack of financial support prevents
any hope of a prolonged life after heart valve replacement.
From criteria pertaining to developing world infrastructure,
surgical expertise and patient lifestyle, a valve was designed
for use in these countries. In order to ensure a successful final
product, the components, materials, assembly and manufacturing
techniques were all chosen to be cost effective and accessible.
The related surgical procedures are simplified so that the risk of
complications is reduced after implantation by surgeons.
Mechanical pericardium tests were performed to understand
whether there was an association between thickness and
tensile strength. It was found that for unfixed pericardium,
tensile strength increased with an increase in tissue thickness.
This motivated an appropriate choice of pericardium in the
valve assembly, offering sufficient residual tensile strength to
successfully undergo the millions of cycles of testing.
Novel heart valve design features, which had not been
implemented in valve designs before or patented in any country
prior to this study, were integrated into this valve design. These
included the use of a mechanical clipping device between the
valve assembly and receptacle, which allowed the surgeon to first
stitch in the sewing ring and then secure the valve and leaflet
assembly in place. This would further permit less-experienced
surgeons to perform valve replacements, with a reduction in risk
of complications.
Attractive benefits offered in this valve design addressed the
issue of re-operation in patients having received a valve implant
in their youth. The valve could easily be swapped for new
leaflets, clipping back into the receptacle without removing it
from the natural valve annulus. This is complemented by the fact
that glutaraldehyde-treated pericardium tissue valves give these
patients freedom from ongoing anticoagulation medication.
Although the design of the valve addressed the technical
aspects of constraint in a theoretical approach, further work
would be required to understand the valve functioning in
a simulated and fatigue-testing environment. As a result of
findings in these areas, a final product could be made available
for commercial use.
References
1.
Carpentier A, Lemaigre G, Robert L, Carpentier S, Dubost C.
Biological factors affecting long-term results of valvular heterografts.
J
Thorac Cardiovasc Surg
1969;
58
(4): 467–483.
2.
Starr A, Edwards ML. Mitral replacement: clinical experience with a
ball-valve prosthesis.
Ann Surg
1961;
154
: 726–740.
3.
Bjork VO. Aortic valve replacement with the Bjork-Shiley tilting disc
valve prosthesis.
Br Heart J
1971;
33
(Suppl): 42–46.
4.
Emery RW, Mettler E, Nicoloff DM. A new cardiac prosthesis: the St.
Jude Medical cardiac valve: in vivo results.
Circulation
1979;
60
(2,
Part 2): 48–54.
5.
Unger F, Ghosh P. International cardiac surgery.
Semin Thorac
Cardiovasc Surg
2002;
14
(4): 321–323.
6.
Blackstone EH. Could it happen again? The Bjork-Shiley convexocon-
cave heart valve story.
Circulation
2005;
111
(21): 2717–2719.
7.
Klepetko W, Moritz A, Mlczoch J, Schurawitzki H, Domanig E,
Wolner E. Leaflet fracture in Edwards-Duromedics bileaflet valves.
J Thorac Cardiovasc Surg
1989;
97
(1): 90–94.
8.
Human P, Zilla P. Characertisation of the immune response to valve
bioprostheses and its role in primary failure.
Ann Thorac Surg
2001;
71
(5, Supple); S385–388.
9.
Vincentelli A, Latremouille C, Zegdi R, Shen M, Lajos P, Chachques J,
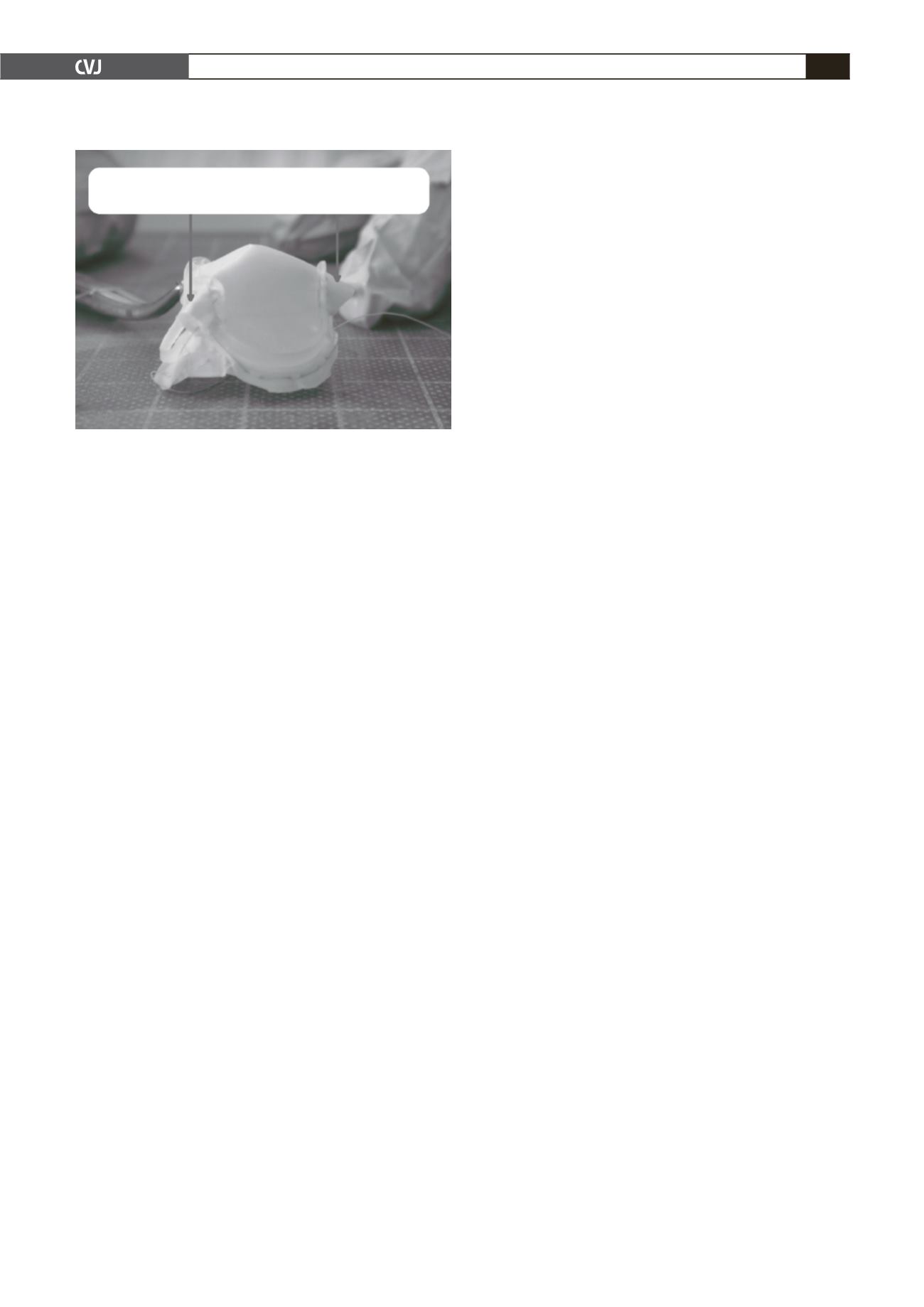
Fig. 3. A fully assembled valve constituted from upper
and lower frame supporting pericardial leaflets.
Leaflet material protruding through the post gap.
To be secured with a hemaclip.


