

















 11 / 74
11 / 74

CARDIOVASCULAR JOURNAL OF AFRICA • Volume 25, No 5, September/October 2014
AFRICA
205
in order to characterise the features of HF and to tailor future
interventions. We also aimed at assessing access to invasive
interventions and outcomes in patients with surgical indications.
Methods
Study setting
The study was conducted at the St Raphael of St Francis
Nsambya Hospital, a tertiary, non-profit hospital with a capacity
of 361 beds, located in urban Kampala. Uganda has a population
of 33 425 000 and a life expectancy of 48 and 57 years in males
and females, respectively
(http://www.who.int/countries/uga/en/)]. The Italian association Solidarity Among People (AISPO),
a non-governmental organisation (NGO) managed by the San
Raffaele Scientific Institute in Milan, Italy, conducted the project
in co-operation with local medical staff.
The main objectives of the project were to gather
epidemiological data on HF in Uganda, and to train Ugandan
doctors, with a special focus on echocardiographic skills. The
present study was conducted during seven NGO missions
(cumulative period of 36 weeks from 2009 to 2013). The
seventh mission was performed in 2013 in order to follow up
on patients who had undergone surgery and those still on the
waiting list. Patients were systematically evaluated by clinical and
echocardiographic examination.
Study cohort
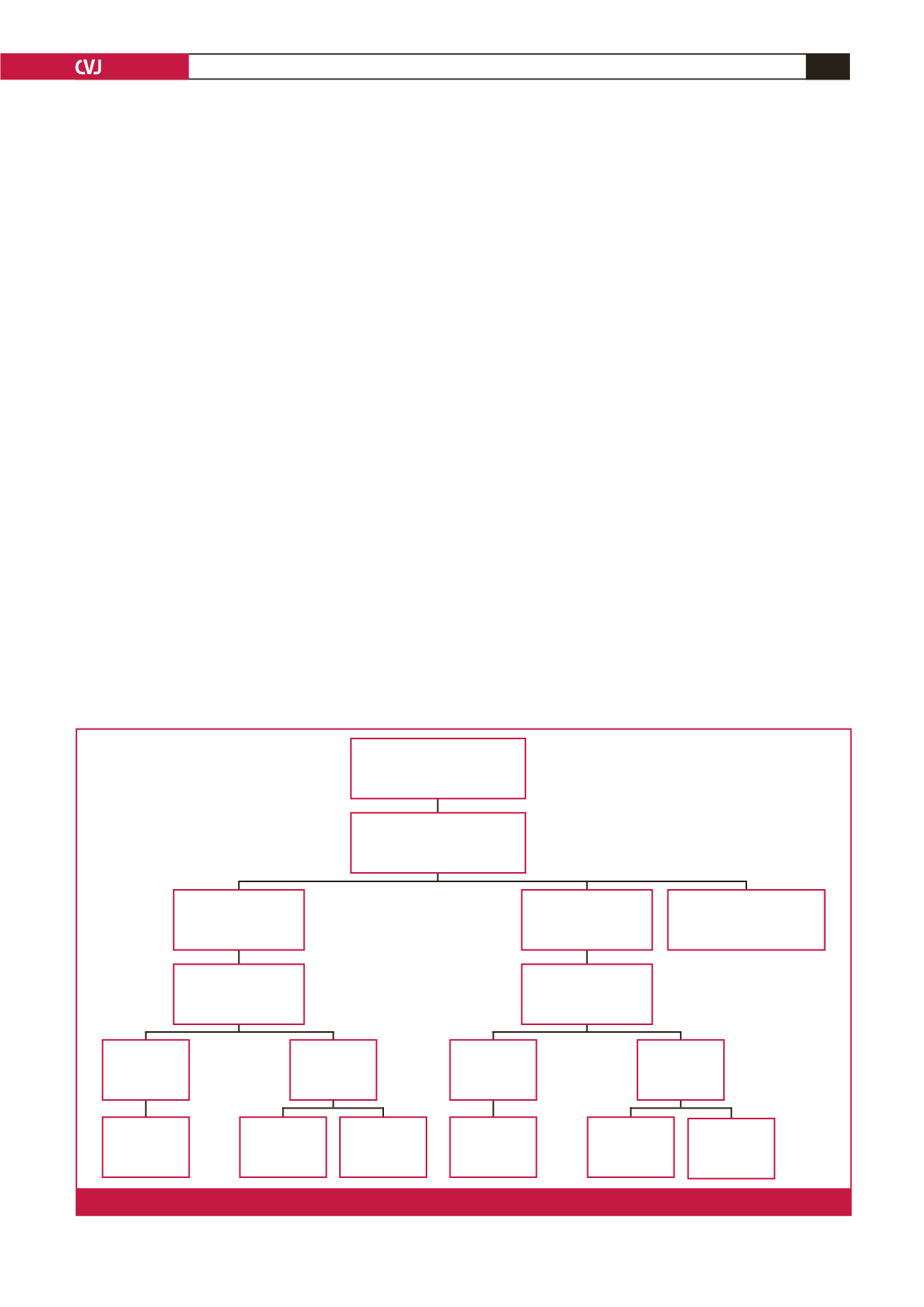
We prospectively studied 272 consecutive subjects [median
age 35 years, interquartile range (IQR) 17–58; 59% female]
referred to the St Raphael of St Francis Nsambya Hospital for
suspected heart disease. Patients were evaluated by clinical and
echocardiographic examination. Electrocardiogram, chest X-ray,
chest computerised tomography (CT) scan and venous Doppler
examination of the inferior limbs were performed as needed.
We studied 160 out-patients (59%) and 112 in-patients
(41%) from the general medical and paediatric wards. In the
study population, 149 patients (55%) were female and 75 (27%)
were children (
≤
16 years). Shortness of breath was the most
frequent motive for seeking medical assistance (
n
=
114, 42%).
One hundred and ninety-seven patients (72%) presented with
structural heart disease, among which 140 (71%) were in clinical
HF.
13
The latter constituted the study cohort (Fig. 1).
Echocardiographic evaluation and study definitions
Italian cardiology teams from the San Raffaele Scientific
Institute in Milan carried out the echocardiograms. General
Electric
®
Logic P5 machines with colour Doppler and two
available probes (1.5–3.5 MHz for adults and 3–8 MHz for
children) were used. Two experienced cardiologists reviewed all
echocardiograms for definite diagnosis (AG and EA).
The aetiology of HF was assessed according to the European
Society of Cardiology guidelines.
13
HF was defined as systolic
HF when left ventricular ejection fraction (LVEF) was
<
50%;
preserved ejection fraction HF when signs of increased left
ventricular filling were detected; and right ventricular HF when
the right ventricle was primarily affected or dysfunctional due
to pulmonary hypertension (PH) not associated with left-sided
heart abnormalities.
Ischaemic heart disease (IHD) was suspected when clear
wall motion abnormalities were observed (there was no cardiac
Patients referred for
echocardiogram
n
= 272
RHD
n
= 44
Yes
n
= 14
Mortality at
FU
n
= 3
Mortality at
FU
n
= 0
Mortality at
FU
n
= 8
Mortality at
FU
n
= 5
Lost to FU
n
= 11
Lost to FU
n
= 8
Yes
n
= 13
No
n
= 30
No
n
= 28
CHD
n
= 41
Other causes: HTN
(
n
= 22), IHD (
n
= 14),
EMF (
n
= 8), PH (n = 7)
Patients with HF due to
structural heart disease
n
= 140
Surgery performed
Surgery performed
Fig. 1.
Flow chart and surgical treatment in patients with rheumatic and congenital heart disease. FU = follow up