
















 65 / 68
65 / 68

CARDIOVASCULAR JOURNAL OF AFRICA • Volume 26, No 6, November/December 2015
AFRICA
e11
femoral artery was conducted. A 5-F pigtail catheter was
inserted into the ascending aorta through the right brachial
artery. This artery was chosen to facilitate proximal imaging, as
delivery of the catheter through the left brachial artery could
have been inhibited by the presence of the thoracic aortic stent
placed six months previously.
Contrast imaging of the aortic arch revealed the
brachiocephalic truncus sourced from the left common carotid
artery (Fig. 3) (bovine arch). Moreover, the origin of the
retrograde dissection flap was identified 1 cm distal to the left
subclavian artery in the contrast view (Fig. 3).
Following the completion of the measurements, a 40
×
212-mm tube stent–graft was implanted into the descending
aorta, including the proximal subclavian section. The placement
of the tube stent–graft was challenging because of the narrowing
of the true lumen and the high-angled aortic progression.
The graft was placed using forced external manoeuvres. An
extension tube stent–graft with a diameter of 42
×
112 mm was
placed through the right common femoral artery. The correct
placement of the extension tube stent–graft was confirmed with
angiography and the application was concluded (Fig. 4). Primary
repair of the right common femoral artery was conducted.
After surgery, no pulse deficit was observed in the left
limb. The patient recovered in the intensive care unit and
hydration was administered for deficient blood urine nitrogen
and creatinine levels (due to the patient’s nephrectomy history).
She was discharged on the fourth day after surgery.
Discussion
All current treatment strategies for AD are associated with a
high mortality rate. This risk is further increased by the extended
patient transfer times. However, recent advances in surgical
procedures may improve the overall morbidity and mortality
rates in AD.
2,3,5
In the present case, a brachiocephalic truncus in
the left common carotid artery (bovine arch) was detected by
contrast-enhanced computed tomography.
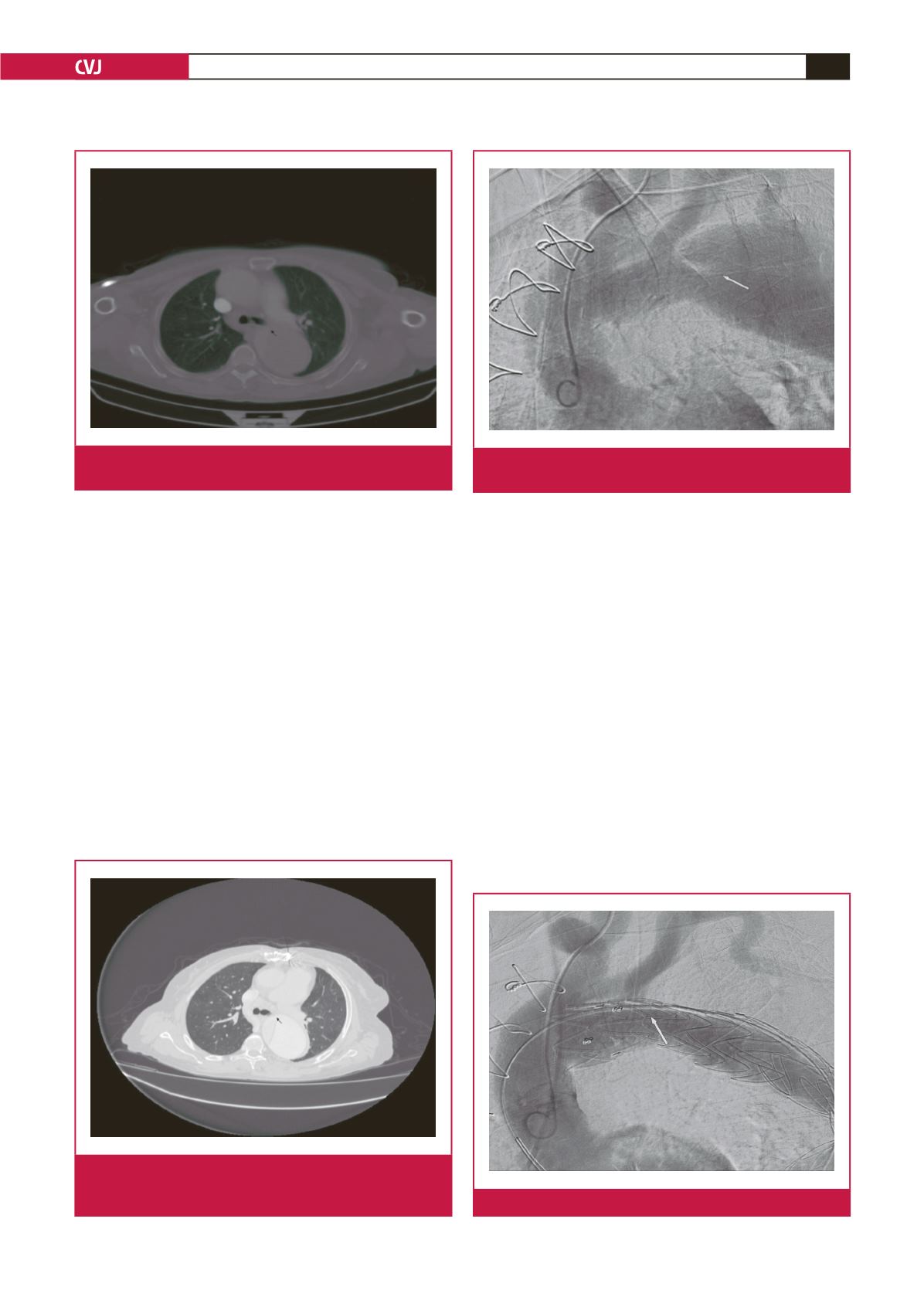
Fig. 1.
Dissection flap without tear during the initial diagnosis
of type A AD.
Fig. 3.
View of the flap tear on the distal side of the subclavian
artery.
Fig. 2.
Dissection flap with tear (flow can be observed
between the true and false lumen) nine months after
replacement of the ascending aorta.
Fig. 4.
Closed flap tear after TEVDAR application.