















 27 / 72
27 / 72

CARDIOVASCULAR JOURNAL OF AFRICA • Volume 27, No 2, March/April 2016
AFRICA
81
Several scoring systems are used to risk stratify women
contemplating pregnancy. The most commonly used are the
cardiac disease in pregnancy (CARPREG) score, the ZAHARA
(Zwangerschap bij Aangeboren Hartafwijking) score, and the
WHO classification, which offer categories of risk.
12
Class IV in
the WHO score is extremely high risk, which contra-indicates
pregnancy. Class IV includes: pulmonary hypertension, severe
systemic ventricular dysfunction, dilated aortopathy and severe
left-sided obstructive lesions.
6
PPC must evaluate the potential
risk posed by pregnancy to the woman, and include information
regarding smoking, anticoagulation and anaemia, medication
and recurrence of congenital heart defects in offspring.
Late presentation of left-to-right shunts in the African setting
often results in Eisenmenger syndrome or pulmonary vascular
disease, associated with cyanosis. Eisenmenger syndrome is
associated with a high maternal and foetal risk, so the affected
should be advised against pregnancy. Specialist counselling
and contraceptive advice are essential to their care. Although
treatment has improved, the maternal mortality rate remains in
excess of 20% in developed countries, and probably closer to 50%
in African settings.
13
Unoperated tetralogy of Fallot is commonly found in Africa in
association with cyanosis and severe right ventricular hypertrophy
and significant antenatal risks. The most common left-sided
lesion is coarctation of the aorta, which is usually repaired in
the neonatal period. Because of late complications, such patients
need lifelong surveillance due to high rates of hypertension, the
need for re-intervention and decreased survival rates.
14,15
Unoperated coarctation may cause severe hypertension, which
can complicate pregnancy. Management of the hypertension
may be difficult and reduction of maternal upper-body blood
pressure may compromise the foeto-placental unit. These
present significant challenges to the cardio-obstetric and cardio-
anaesthetic teams, so they are best managed before conception,
with individualised patient-care plans, based on their anatomy
and physiology.
16
All patients with known cardiac disease should preferably be
counselled before conception. Pre-pregnancy evaluation should
include a comprehensive risk assessment for the mother and foetus,
including medication use and information on heredity of the
cardiac lesion. In cases of late diagnosis of congenital heart disease,
combined with limited specialised cardiac resources, PPC is crucial
to assessing pregnancy risks. Safe contraception options should be
considered with a multidisciplinary management team. Continued
attention should remain on the critical elements of PPC, such as
nutritional support, family spacing and genetic conditions.
Rheumatic heart disease
Rheumatic heart disease remains an endemic condition on the
African continent, with an incidence of 27 per 100 000,
17
and
a prevalence of over 20 per 1 000 in sub-Saharan Africa.
18,19
Moreover, recent studies demonstrate the severity of the disease
in tertiary institutions in Africa, with the majority of cases
presenting with established heart failure, atrial fibrillation and
pulmonary hypertension.
20,21
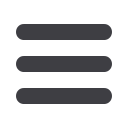
The pathognomonic lesion in established rheumatic heart
disease is mitral stenosis, which is associated with complications
such as atrial fibrillation, stroke and death (Fig. 1). Valvular heart
disease, especially stenotic valvular lesions, results in significant
physiological effects during pregnancy, and is associated with
maternal mortality and foetal loss.
22,23
A previous study of
46 pregnant Senegalese women with rheumatic heart disease
reported 17 maternal deaths (34%), six foetal deaths, and five
therapeutic abortions.
24
Severe mitral stenosis is classified as extremely high risk,
therefore contra-indicating pregnancy. It is critical to evaluate all
women of childbearing age with severe mitral stenosis, in order
to provide family planning advice. In cases where pregnancy
is strongly desired, pre-pregnancy interventions should be
considered.
25
Although mitral regurgitation is better tolerated
during pregnancy, patients with severe symptomatic mitral
regurgitation and impaired left ventricular function should be
considered for timely surgery.
26
Two final scenarios must be considered. The first scenario is
the woman with a prosthetic heart valve desirous of pregnancy.
Clear information on choices of anticoagulation therapy (e.g.
heparin, warfarin or enoxaparin) during a potential pregnancy
should be discussed with health professionals, with a clear plan
to prevent complications and mortality.
27
The second scenario
is the patient with moderate mitral stenosis and a dilated left
atrium, which increases the risk of stroke due to the lesion and
the pregnant state.
28
Once again, treatment options should be
discussed prior to conception.
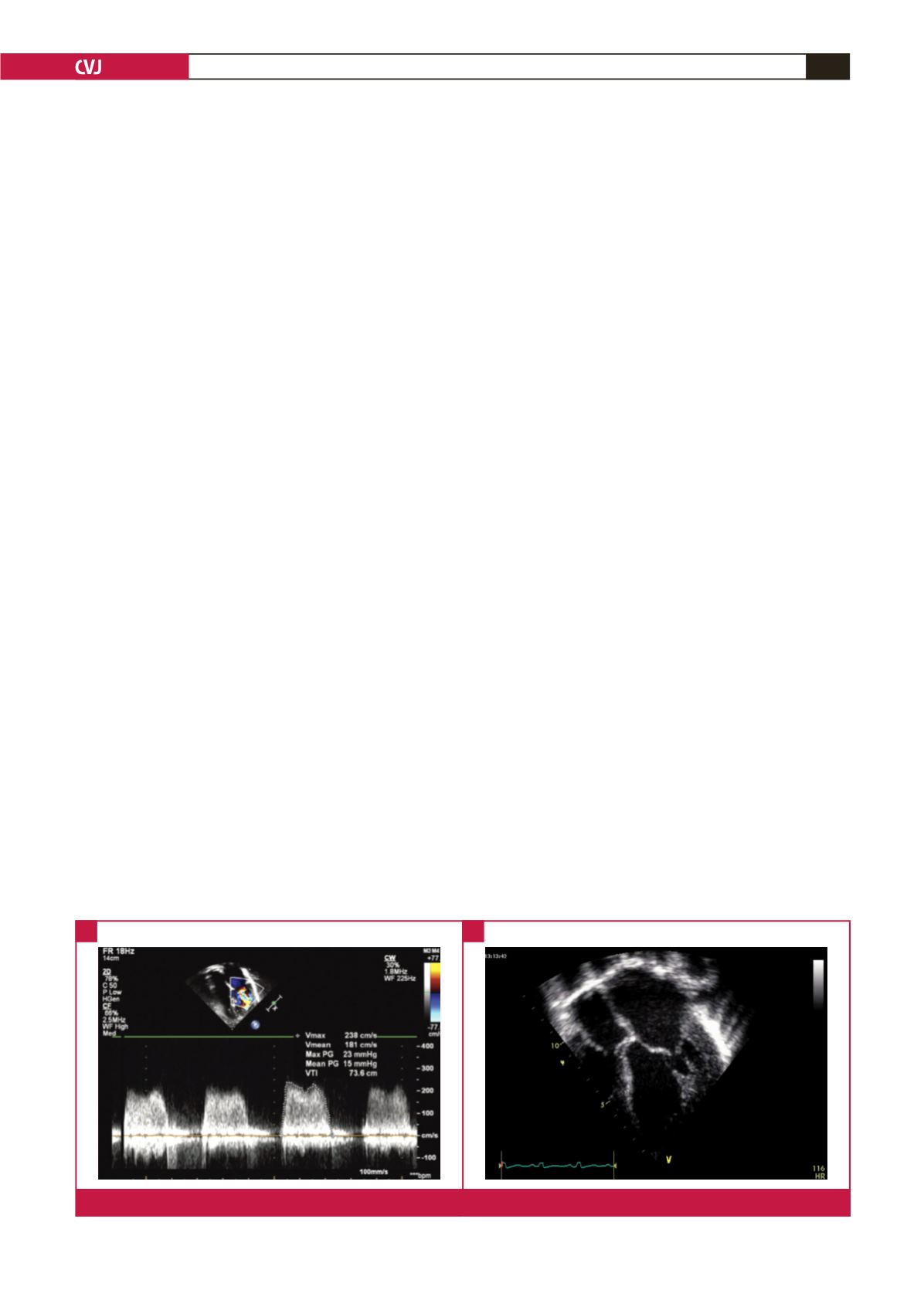
Fig 1.
Severe mitral stenosis (A) Doppler echocardiography; mean gradient 15 mmHg and (B) dilated left atrium with reduced excursion.
A
B