CARDIOVASCULAR JOURNAL OF AFRICA • Vol 24, No 6, July 2013
202
AFRICA
Cardiovascular Topics
Ductal closure using the Amplatzer duct occluder type
two: experience in Port Elizabeth hospital complex,
South Africa
LUNGILE PEPETA, ADELE DIPPENAAR
Abstract
Objective:
To report outcomes in percutaneous ductal closure
using the Amplatzer duct occluder type two (ADO II).
Methods:
Records of patients admitted for percutaneous
closure of patent ductus arteriosus (PDA) were reviewed.
Results:
From May 2009 to July 2012, 36 patients were
assigned to closure using the ADO II. There were 21 females
and 15 males. The median age was 16.5 (2–233) months;
median weight, 8 (3.94–39.2) kg; and median height, 75
(55–166) cm. The mean pulmonary artery pressure was 24.4
(
±
10.4) mmHg, the pulmonary blood flow:systemic blood
flow (Qp:Qs) ratio was 2.25 (
±
1.97), and mean pulmonary
resistance (Rp) was 1.87 (
±
1.28) Wood units. The mean
ductal size was 2.74 (
±
1.3) mm. In 30 patients the device
was delivered through the pulmonary artery. Thirty-three
patients achieved complete closure by discharge (day one).
Conclusion:
The ADO II is capable of closing a wide range of
ducts in carefully selected patients. Our findings are compa-
rable with other studies regarding ductal closure rates.
Keywords:
patent ductus arteriosus, Amplatzer duct occluder II,
percutaneous ductal closure
Submitted 2/11/12, accepted 10/5/13
Published online 27/6/13
Cardiovasc J Afr
2013;
24
: 202–207
DOI: 10.5830/CVJA-2013-033
The incidence of patent ductus arteriosus (PDA) accounts for
11.9 to 15.6% of all congenital heart diseases.
1,2
This figure rises
to about 31% in premature infants.
3
Surgical closure of the PDA
was first reported by Gross,
et al
. in 1938.
4
However, it was not
until 1967 when Porstmann,
et al
. reported the first percutaneous
closure of the PDA in the cardiac catheterisation laboratory.
5
Several devices have been introduced for transcatheter closure of
the PDA over the years.
6-16
In 2008, the Amplatzer duct occluder
type two (ADO II) (St Jude Medical, Cardiovascular Division, St
Paul, MN) was introduced.
17
We report on our experience from
a single centre.
Methods
Following ethics clearance, a review of records of patients who
underwent percutaneous closure of the PDA in the Port Elizabeth
Provincial Hospital, Port Elizabeth, South Africa was performed.
Patients’ age, gender, weight, pulmonary blood flow:systemic
blood flow (Qp:Qs) ratios, and pulmonary resistance (Rp)
were documented. Angiographic anatomy, including narrowest
diameter (ductal size), ductal length and ductal ampulla; selection
of ductal closure device; ductal closure approach; radiological
screening time; complications and outcomes were also noted.
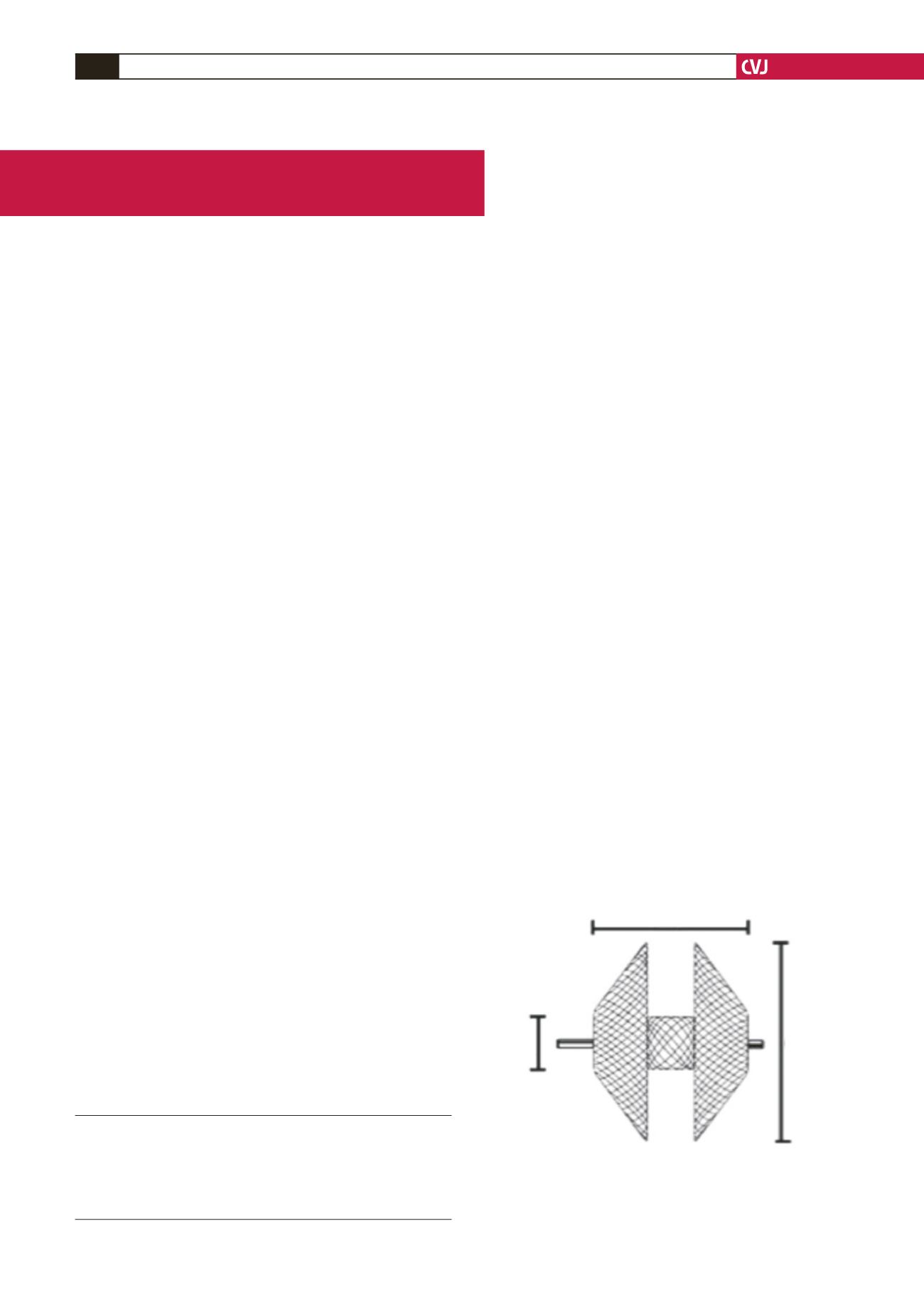
The Amplatzer duct occluder type two device is made of a
meshwork of self-expandable nitinol wire. It consists of a central
‘lobe’, which measures 3–6 mm in diameter, and two retention
disks on either side of the lobe (Fig. 1). The disks are 6 mm
larger than the central lobe and range from 9–12 mm in diameter.
The devices are designed in such a way that the central lobe is
the one that is placed in the duct itself, with a retention disk on
either side of the PDA.
The device is delivered using a TorqVue low-profile (LP)
delivery system (Fig. 2). The reason these newer devices can be
delivered using a low-profile delivery system is that they lack the
polyester material that is present in the Amplatzer duct occluder
Division of Paediatric Cardiology, Paediatrics and Child
Health, Dora Nginza Hospital, Port Elizabeth, Eastern Cape
South Africa
LUNGILE PEPETA, FCPaed (SA), Cert Cardiol (SA), Lungile.
ADELE DIPPENAAR, FCPaed (SA), MRCPCH (UK)
Fig. 1. Amplatzer duct occluder type II device. A. Central
lobe diameter (3–6 mm), B. Device length (4 or 6 mm),
C. Retention disks diameter (9–12 mm). (Figure used
with permission from St Jude Medical, Cardiovascular
Division, St Paul, MN).
A
B
C


