CARDIOVASCULAR JOURNAL OF AFRICA • Vol 23, No 8, September 2012
AFRICA
e17
The anomaly in which the isolated LAD originates from
the pulmonary artery is more rare than the classic ALCAPA
syndrome. In this type of coronary artery anomaly, ischaemic
risk is constituted by the low perfusion pressure in the LAD
region. The right coronary and circumflex arteries may also be
highly ectasic and send collaterals to the LAD.
5
In this anomaly, the only symptommay be atypical angina, and
systolic murmur can only be detected in a physical examination.
Neither was present in our case, however, sudden cardiac arrest
developed during exercise and cardiopulmonary resuscitation
was performed. The patient had developed ventricular fibrillation,
was defibrillated and returned to sinus rhythm.
In the ALCAPA syndrome, while there may be changes in
the ECG such as left ventricular hypertrophy, left electrical axis
deviation, and anterolateral wall infarction, the ECG may be also
entirely within normal limits.
6
In our case, the ECG was in sinus
rhythm and had a T-wave negativity in V
1
–
V
2
derivation.
The diagnosis of coronary artery anomalies with TTE is
difficult because it may not always be possible to show the origins
of the coronary arteries in adult patients; it is easier in newborns.
In some cases, the anomalous origin of the left coronary system
as well as the retrograde flow into the pulmonary artery may be
seen directly.
7
If there is a strong clinical or echocardiographic-
based suspicion about the existence of this anomaly, then
coronary or CT angiography should definitely be performed.
In our case, we could not reach an exact diagnosis with TTE,
as only an increase in the left ventricular wall thickness and
slight expansion in the left ventricle were detected. However,
colour Doppler examination showed intra-myocardial blood flow
with a retrograde flow inside the pulmonary artery, which we had
not expected.
We suspected there might be a coronary artery anomaly in
the patient and performed coronary and CT angiography. The
sensitivity of an angiography may be limited in the diagnosis
of an anomalous coronary artery due to its invasive nature.
CT angiography is a valuable non-invasive method to show
abnormal coronary arteries, their origins and projections, and it
indicates a prognosis of the coronary arteries.
8
Due to the coronary steal phenomenon that occurs during
exercise, arrhythmias can be triggered because of inadequate
myocardial perfusion. In our case, ECG and TTE did not
indicate previous myocardial infarction. There was no increase
in troponin I values; however, in the cardiac MRI, we identified
a sub-endocardial infarct in the apical and antero-septal regions,
which we had not been able to identify with TTE. Left ventricular
dysfunction, significant mitral regurgitation and pulmonary
hypertension were not present in our case. However, cardiac
arrest had developed during exercise.
In patients with ALCAPA syndrome, even if the patient is
asymptomatic, or when ventricular arrhythmia and significant
left-to-right shunt or risk of death is not present, surgical
treatment is suggested.
9
In the past, several methods such as
binding of the pulmonary artery or aorto-pulmonary anastomosis
have been used in the treatment of ALCAPA syndrome in the
elderly.
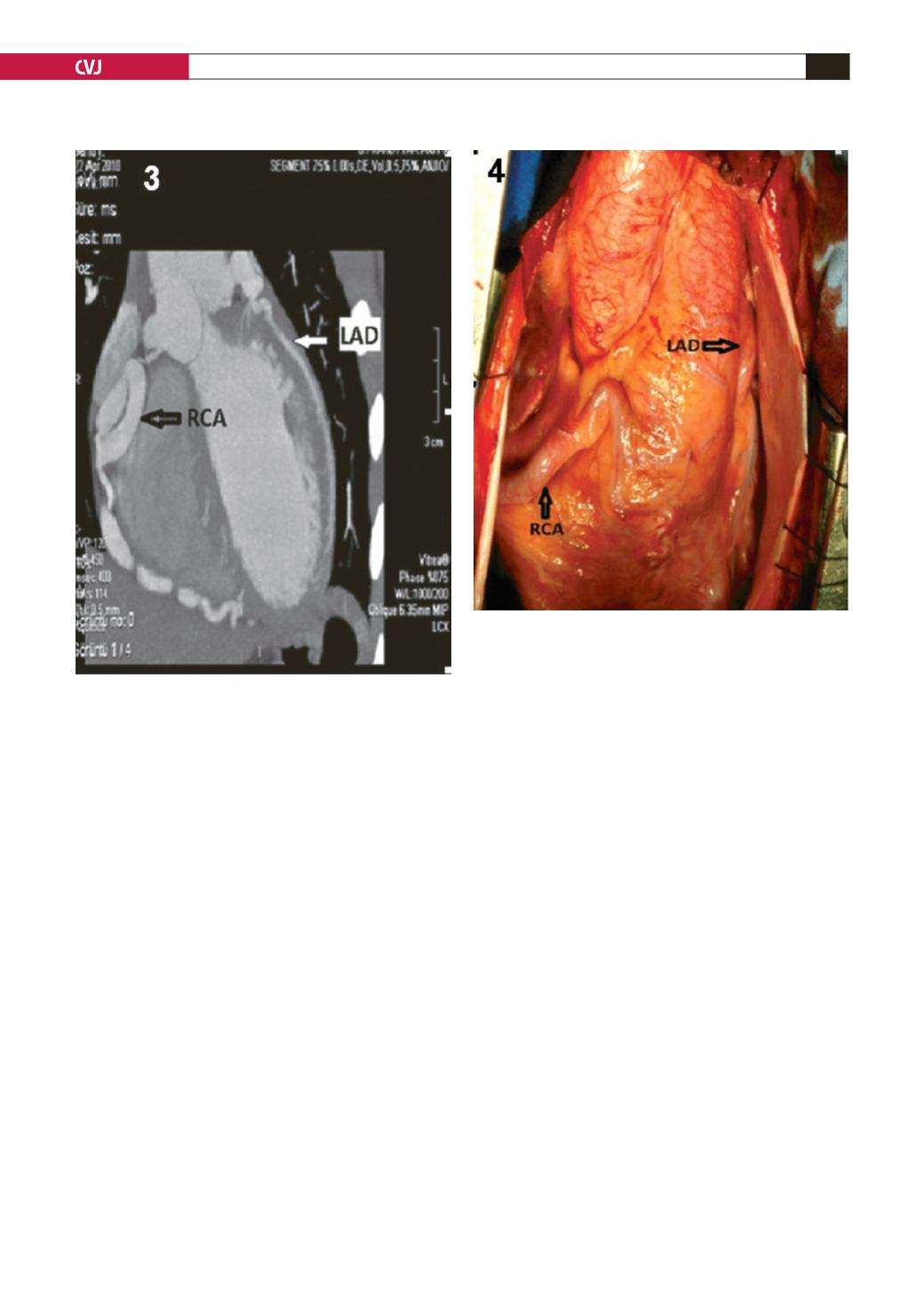
Fig. 4. After the pericardium was opened during surgery,
the RCA was seen to be ectatic and curly, similar to the
coronary angiographic image. The LAD was ectatic and
collaterals ran between it and the RCA. RCA: right coro-
nary artery, LAD: left anterior descending artery.
Fig. 3. Longitudinal image with CT angiography showing
the right coronary artery originating from the aorta, and
the LAD originating from the pulmonary artery. RCA: right
coronary artery, LAD: left anterior descending artery.


