

















 54 / 67
54 / 67

CARDIOVASCULAR JOURNAL OF AFRICA • Vol 24, No 2, March 2013
e4
AFRICA
Case Report
Is a drug-challenge test with propafenone adequate to
exclude Brugada syndrome?
BEKİR SERHAT YİLDİZ, HASAN GUNGOR, ILKER GUL, MURAT BİLGİN, MEHDİ ZOGHİ, AZEM AKİLLİ
Abstract
Brugada syndrome is associated with sudden cardiac death
in patients with a structurally normal heart. The electrocar-
diogram (ECG) pattern of Brugada syndrome is character-
ised by complete or incomplete right bundle branch block
and ST-segment elevation in the right precordial leads. These
ECG signs may not always be apparent but can be unmasked
with certain anti-arrhythmia agents. We report here a case
of a 26-year-old woman without detectable structural heart
disease but with a history of syncope, cardiac arrest, intu-
bation and defibrillation for ventricular fibrillation. We
performed challenge tests with propafenone and ajmaline.
After infusion of propafenone, there were minimal ECG
changes which were not diagnostic for Brugada syndrome.
One week later the provocation test was repeated with
ajmaline. During infusion of ajmaline, prominent J waves
and ST-segment elevation appeared in the right precordial
leads (V1–3). Premature ventricular complexes were seen on
a 12-lead ECG. The patient’s ECG showed Brugada type 1
pattern. She received an internal cardioverter/defibrillator
and was discharged with a beta-blocker.
Keywords:
Brugada syndrome, propafenone, ventricular fibril-
lation
Submitted 28/8/12, accepted 4/10/12
Published online 13/11/12
Cardiovasc J Afr
2013;
24
: e4–e6
www.cvja.co.zaDOI: 10.5830/CVJA-2012-068
Brugada syndrome (BS) is characterised by complete or
incomplete right bundle branch block (RBBB) pattern with
ST-segment elevation in leads V1–3 and a propensity for episodes
of sudden cardiac death or syncope caused by life-threatening
cardiac arrhythmias in a structurally normal heart.
1,2
The clinical
presentation is distinguished by a male predominance and
the appearance of arrhythmic events at an average age of 40
years.
3
The syndrome is usually identified by a characteristic
Brugada-type ECG that consists of ST elevation of a coved type
in precordial leads V1 to V3, although affected individuals may
have a normal ECG.
4,5
Because patients with BS usually become
symptomatic at a relatively young age, early diagnosis is crucial
to prevent sudden cardiac death (SCD) due to a higher risk of
developing an arrhythmic event.
6
Case report
A 26-year-old woman was admitted to the Department of
Cardiology for dizziness, history of syncope, cardiac arrest
and cardiopulmonary resuscitation (CPR). There was no family
history of sudden death. The patient had a history of syncope
eight years previously while walking, without prodromal signs.
The syncope attack was repeated three weeks prior to admission.
She had had palpitations before the syncope but no chest pain.
She had CPR for 15 minutes and had been intubated. In the
ambulance she had been defibrillated twice with 360 Joules
because of ventricular fibrillation, and was admitted to the
emergency department.
Department of Cardiology, Denizli State Hospital, Denizli,
Turkey
BEKİR SERHAT YİLDİZ, MD,
bserhatyildiz@yahoo.comDepartment of Cardiology, Adnan Menderes University,
Aydin, Turkey
HASAN GUNGOR, MD
Department of Cardiology, Trabzon Ahi Evren State
Hospital, Trabzon, Turkey
ILKER GUL, MD
Department of Cardiology, Diskapi Yildirim Beyazit Training
and Research Hospital, Ministry of Health, Ankara, Turkey
MURAT BİLGİN, MD
Department of Cardiology, Ege University Medical Faculty,
Izmir, Turkey
MEHDİ ZOGHİ, MD
AZEM AKİLLİ, MD
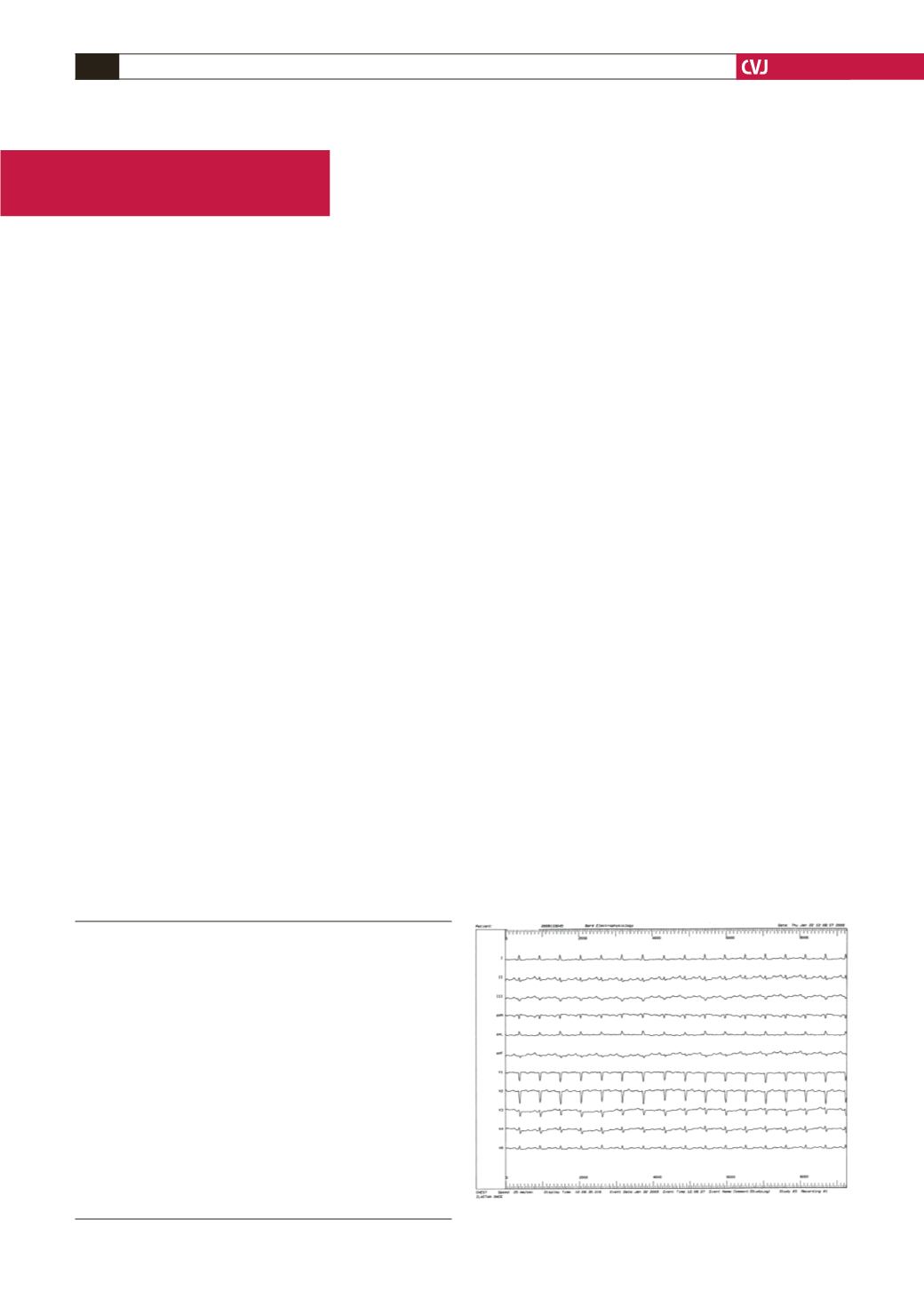
Fig. 1. Basal ECG.