

















 58 / 67
58 / 67

CARDIOVASCULAR JOURNAL OF AFRICA • Vol 24, No 2, March 2013
e8
AFRICA
evidence of peripheral artery disease.
Anticoagulation was started immediately with unfractionated
heparin (UFH), and the patient underwent surgical thrombectomy.
Fresh thrombi were obtained from both popliteal arteries at the
level of bifurcation via a femoral arterial incision (Fig. 1).
Anticoagulant therapy was continued with UFH for three days
and with low-molecular weight heparin (LMWH) at a dosage of
6 000 IU twice daily throughout his hospital stay.
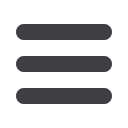
He was discharged uneventfully on the fifth postoperative day
with LMWH treatment (enoxaparin 8 000 IU/day). He was doing
well at the first month’s postoperative follow up, with palpable
distal pulses, warm feet and three-phasic flow characteristics on
the Doppler control (Fig. 2).
Discussion
The incidence of thrombosis in malignancy is rapidly increasing.
Furthermore, malignancy is the second most common cause of
death in patients with peripheral arterial disease. In one study,
the incidence of clinical thrombosis in patients with cancer was
5–17% compared with 0.1% in the general population, most
of which are venous thrombosis.
4
In a recent study, Tsang
et
al.
reported a 3.8% incidence of arterial thrombosis in cancer
patients. Of the 419 patients with acute limb ischaemia, 16 had
associated cancer.
5
Despite many shared risk factors, the association between
arterial thrombosis and malignancies, and the pathogenesis of
thrombosis are not well understood. Goldenberg
et al
. reported an
increase in plasma levels of the thrombin–antithrombin complex
and prothrombin fragments 1 and 2, together with a significant
decrease in protein C activity in cancer patients.
6
Contributing
factors to thrombosis in malignancy include pro-coagulant
and cytokine release from damaged tumour cells, endothelial
damage caused by cytotoxic agents, and decreasing levels of
anticoagulants due to hepatotoxic effects of the chemotherapy
agents.
5
Up to 30 years ago, acute arterial embolismwas usually caused
by atrial fibrillation or mural thrombosis. The atherosclerotic
process is the most common cause of this phenomenon today.
7
However, Tsang
et al
. found that the development of arterial
thrombosis in cancer patients depended mainly on spontaneous
in situ
thrombosis in vessels without any pre-existing vascular
disease, rather than atherosclerosis or other structural vascular
problems.
5
They reported that histological examination of
the thromboembolic material derived from their subjects was
consistent with thromboembolism, and no tumour cells were
identified.
5
They concluded that nearly all acute ischaemic
events, as in our case, are the result of thromboembolus rather
than tumour emboli.
Arterial thrombosis is an uncommon adverse event
following chemotherapy with 5-fluorouracil. In the literature
however, cisplatin was reported as the most common agent of
thromboembolism (8.4–17.6%).
5,8
In some individual case series,
different aetiological agents were referred to, such as bleomicin,
9
cyclophosphamide
4
or methotrexate.
5
When we examined these
studies, we noted that most used multiple chemotherapeutic
agents in combination, rather than one agent.
Heinrich
et al
. reported an aorto-bifemoral embolism
in an 18-year-old patient after cisplatin and 5-fluorouracil
chemotherapy, and treated it with discontinuation of the cisplatin
regimen.
8
However, in our patient, although he had been taking
both 5-fluorouracil and cisplatin, the oncologist considered
5-fluorouracil to be the causative agent of the thrombogenesis
and discontinued this agent. On LMWH treatment, there was
no evidence of thrombosis, and our patient had an almost
totally undamaged vascular wall and normal vascular flow
rate on Doppler ultrasonography. The exact mechanism of the
thrombosis triggered by 5-fluorouracil, however, is unclear.
Optimal management of cancer patients requires a strong
suspicion of an ischaemic event, concurrent with immediate
anticoagulation and surgical intervention. On the other hand, in
patients with acute arterial thrombosis without any history of or
risk factors for peripheral arterial disorder, screening for occult
malignancy should be considered.
5
Conclusion
We present an unusual case on the relationship between
combined chemotherapy and arterial thrombosis. Although there
are conflicting reports in the literature on the origins of thrombi,
combined chemotherapy regimens may be the causative factors.
However tumour-related release of pro-coagulants may also
Fig. 2. Doppler ultrasonographic data of the patient’s first month of follow up.