CARDIOVASCULAR JOURNAL OF AFRICA • Vol 24, No 9/10, October/November 2013
382
AFRICA
Case Report
Ebstein’s anomaly and Down’s syndrome
LUNGILE PEPETA, SALLY-ANN CLUR
Abstract
We report on two cases presenting with a rare combina-
tion of Ebstein’s anomaly and Down’s syndrome. The first
patient presented with respiratory distress, mild cyanosis
and right heart failure immediately after delivery. The symp-
toms improved with heart failure medication. The patient
remained asymptomatic on follow up. The second patient was
diagnosed antenatally with marked apical displacement of
the tricuspid valve and a very small functional right ventricle
compared to the left ventricle. At birth, the patient presented
with an extreme form of Ebstein’s anomaly with severe
cyanosis, marked right heart failure and ductal-dependent
pulmonary blood flow. The patient died within days of birth.
Keywords:
Ebstein’s anomaly, Down’s syndrome, prenatal and
postnatal diagnosis, right heart failure
Submitted 21/8/11, accepted 14/8/13
Published online 5/9/13
Cardiovasc J Afr
2013;
24
: 382–384
DOI: 10.5830/CVJA-2013-054
Ebstein’s anomaly was first described by Wilhelm Ebstein in
1866, in an autopsy report of a 19-year-old patient who had
presented with cyanosis and right heart failure.
1,2
Ebstein’s
anomaly is characterised by significant apical displacement of
the tricuspid valve. It is very rare, with an incidence of 1:20 000
live births, and accounts for less than 1% of all congenital heart
defects.
3
The time of clinical presentation may range from foetal
life to late adulthood, depending on the extent of the tricuspid
valve displacement, size and function of the right ventricle, right
atrial size and degree of right-to-left shunting.
4
By contrast, Down’s syndrome, first described by Seguin
and Down in 1846 and 1866, respectively,
5
is fairly common.
Congenital cardiac lesions occur in 40 to 50% of these patients
and include atrioventricular septal defects, atrial septal defects,
ventricular septal defects, patent ductus arteriosus and tetralogy
of Fallot.
6
We present two cases of a very rare combination of
Ebstein’s anomaly and Down’s syndrome.
Case reports
Case 1
The patient was a female infant delivered at 33 weeks’ gestation,
with a birth weight of 1 980 g andApgar scores of 6 at one minute,
9 at five minutes and 9 at 10 minutes. She had the phenotypic
features of Down’s syndrome and had respiratory distress with
cyanosis. The oxygen saturations were 85% on room air and
98% on nasal prongs oxygen at 2 l/min. Her temperature was
38.8°C. The pulse rate was 170 beats per min (bpm). The blood
pressure was normal. A 3/6 holosystolic murmur over the left
lower parasternal boarder was noted.
The liver was enlarged at 4 cm below the costal margin. The
chest X-ray showed cardiomegaly with a cardiothoracic ratio
of 65%, oligemic lung fields, features of right atrial and right
ventricular enlargement, left aortic arch and situs solitus. The
ECG showed a sinus rhythm with a rate of 165 bpm, PR interval
of 100 ms and QRS axis of –40 degrees. There were tall R waves
in V1 of 15 mm and deep Q waves in aVR, V1 and V2, features
which were suggestive of right ventricular hypertrophy with
strain.
Echocardiography revealed a dilated right side of the heart
(Fig. 1). The septal leaflet of the tricuspid valve was apically
displaced at 7.8 mm below the anterior leaflet of the mitral valve
and was redundant. This displacement when indexed for body
surface area was significant at 49 mm/m
2
. Moderate tricuspid
regurgitation was seen on colour flow Doppler. However,
no tricuspid valve stenosis or right ventricular outflow tract
obstruction was seen. The foramen ovale and ductus arteriosus
were closed. No other cardiac abnormalities were detectable.
Dora Nginza Hospital, Port Elizabeth Hospital Complex, Port
Elizabeth, South Africa
LUNGILE PEPETA, FCPaed (SA), Cert.Cardiology (SA), MMed
(Wits),
Department of Paediatric Cardiology, Emma Children’s
Hospital, Academic Medical Centre (AMC) and Centre for
Congenital Heart Anomalies Amsterdam-Leiden (CAHAL),
The Netherlands
SALLY-ANN CLUR, MB BCh, MSc (Med), FCP (SA) (Paed), PhD
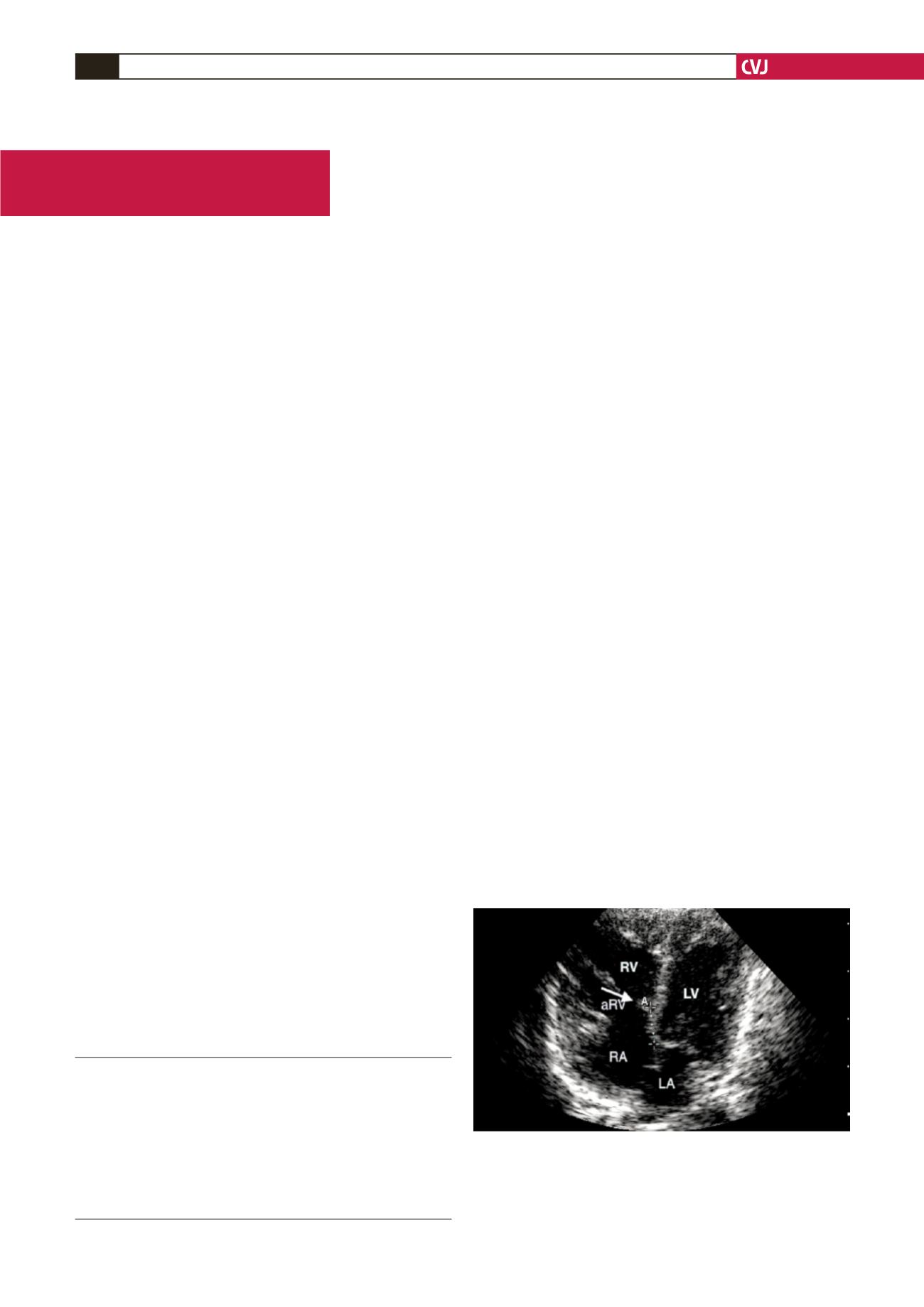
Fig. 1. Two-dimensional echocardiogram in the four-
chamber view of case 1, showing Ebstein’s anomaly with
right atrial dilatation (RA) and apical displacement of the
septal leaflet of the tricuspid valve (arrow), leading to atri-
alisation of the right ventricle (aRV). RV, right ventricle;
LA, left atrium; LV, left ventricle.


