CARDIOVASCULAR JOURNAL OF AFRICA • Vol 24, No 9/10, October/November 2013
AFRICA
e5
addition, she had malaligned dentition and right-ear hearing loss
as part of the OI syndrome.
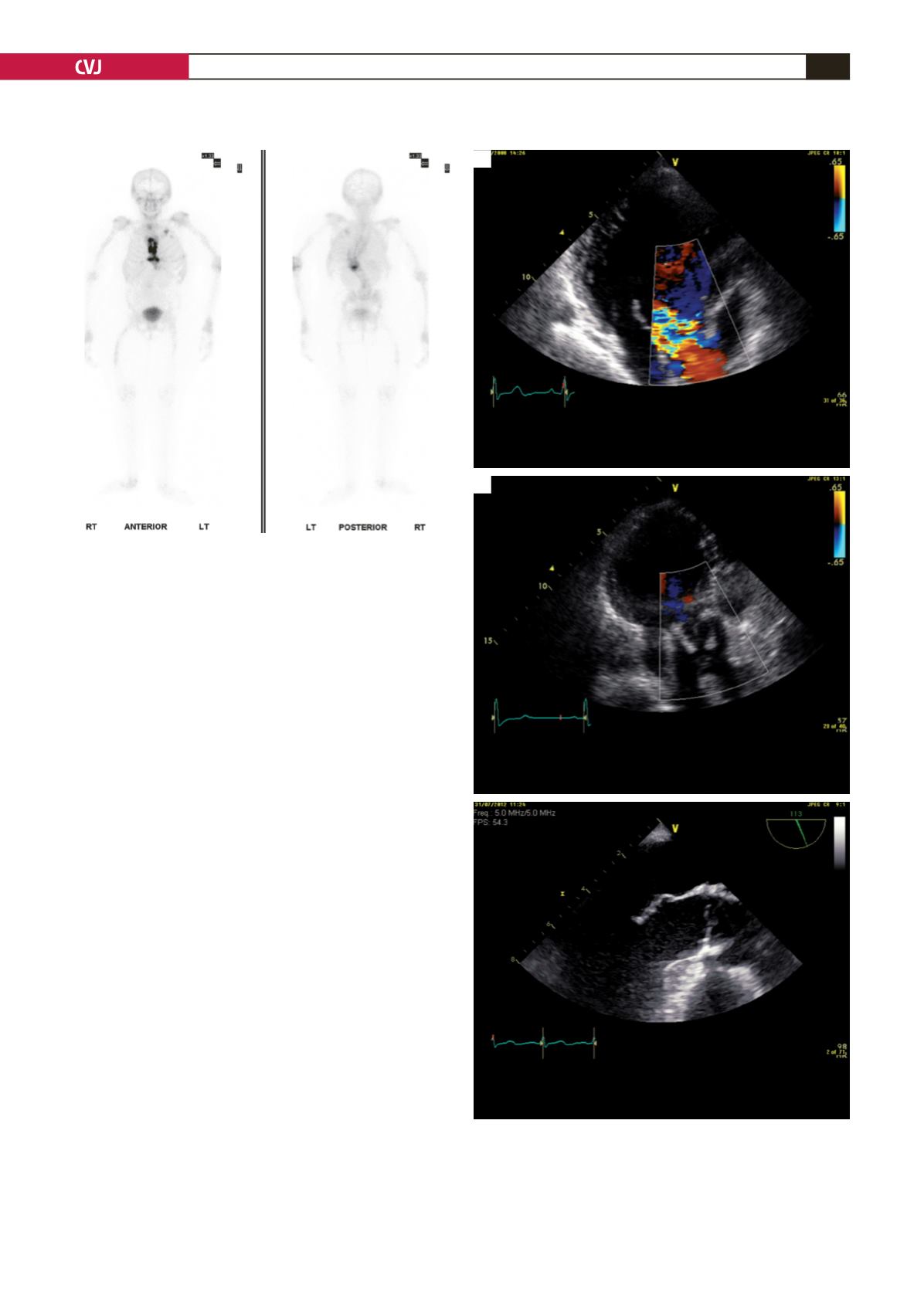
The patient presented with progressively increasing dyspnoea
(NYHA III) over the previous 12 months and transthoracic
echocardiography confirmed severe aortic valve regurgitation
(Fig. 3). A CT coronary arteriogram showed no coronary
artery disease and her predictive operative mortality (logistic
EuroSCORE) was 4.7%.
We elected to use a mini-sternotomy approach with an
inverted T incision in order to maintain chest cage integrity.
Cardiopulmonary bypass was established with cannulation of the
ascending aorta using an aortic cannula (Seldinger’s technique)
along with a single venous cannula. A hockey stick aortotomy
was used and direct cold blood cardioplegia was given through
the coronary ostia.
An aortic valve replacement (Medtronic-Mosaic 25 mm)
with pledgeted, supported and non-everted sutures was done
uneventfully (cross-clamp time 62 min; perfusion time 81 min).
All these manoeuvres were performed to minimise surgical
trauma during the procedure. BioGlue was used to reinforce the
aortotomy suture line and cannulation sites. Two units of platelets
plus four units of fresh, frozen plasma were transfused after
weaning from extra-corporeal circulation.
The patient made an uneventful recovery and was discharged
on the eighth postoperative day. At 36 months’ follow up, the
patient was doing well. Histological sections of the aortic valve
demonstrated myxoid degeneration and the morphology of the
aortic wall was normal.
Discussion
The first report of the term OI was by Olaus Jakob Ekman
in a doctoral thesis for the University of Uppsala in 1788. He
described a family where three generations of people had a
condition that he termed ‘osteomalacia congenita’.
2
The severity of the disease is proportional to the quality of
the mutation and the extent of the abnormal type I collagen. The
percentage of OI patients requiring cardiac surgical treatment
Fig. 3. A: pre-operative echocardiography. B: postopera-
tive echocardiography.
A
B
Fig. 2. Postoperative radioisotope bone scan. There
is increased uptake in the upper part of the sternum,
however, there is no evidence of recent rib fracture.


