CARDIOVASCULAR JOURNAL OF AFRICA • Vol 24, No 9/10, October/November 2013
AFRICA
e9
clinical episodes of arterial, venous, or small-vessel thrombosis
in any tissue or organ, confirmed by findings from imaging
studies, Doppler studies, or histopathology and/or pregnancy
mortality, premature births, spontaneous abortions and stillbirth.
The laboratory criterion outlines that patients must have
(1) medium to high levels of immunoglobulin G (IgG) or
immunoglobulin M (IgM), anticardiolipin (aCL), anti-beta-2
glycoprotein I, or LA on at least two occasions at least 12 weeks
apart. Other criteria include cardiac valve vegetations (Libman-
Sachs endocarditis), valvular insufficiency, livedo reticularis,
leg ulcers, migraine headaches, and a variety of neurological
complications, including chorea and transverse myelopathy.
1
The antiphospholipid syndrome can be primary or secondary
depending on the presence or absence of autoimmune diseases,
viral infections, cancer, but more commonly systemic lupus
erythematosis.
Epidemiological studies have shown that antiphospholipid
antibodies are found among young, apparently healthy control
subjects at a prevalence of 1–5% for both anticardiolipin
antibodies and lupus anticoagulant antibodies.
12
The prevalence
of antiphospholipid antibodies increases with age, especially
among elderly patients with coexisting chronic diseases.
12
Many patients have laboratory evidence of antiphospholipid
antibodies without clinical consequences. In apparently healthy
control subjects, there are insufficient data to determine
what percentage of those with antiphospholipid antibodies
will eventually have a thrombotic event or a complication
of pregnancy consistent with the antiphospholipid syndrome.
In contrast, the antiphospholipid syndrome may develop in
50–70% of patients with both systemic lupus erythematosus and
antiphospholipid antibodies after 20 years of follow up.
12,13
The modality of treatment depends on the pattern of
presentation. Aspirin and hydroxychloroquine are used in
prophylaxis, warfarin is prescribed for prevention of further
thromboses of large vessels and a combination of anticoagulants
and steroids plus either plasmapheresis or intravenous immune
globulin are effective in acute thrombotic microangiopathy.
Currently, heparin administered to pregnant women with
antiphospholipid syndrome after ultrasonographic demonstration
of a live embryo is the treatment of choice.
11
Case report
A 21-year-old female Nigerian of Igbo ethnicity presented
at the medical outpatient department of the University of
Nigeria Teaching Hospital, Ituku-Ozalla, Enugu, with high-
grade intermittent fever for seven weeks and symmetrical
polyarthralgia for 10 days. The fever had resolved by the time
she was evaluated in our centre. The patient was unmarried
and her gyneco-obstetrical history was uneventful, with regular
menstruation. She was not on oral contraceptives and does not
smoke. She is not a known diabetes mellitus patient. She noted
some numbness and discoloration of the toes. There was also
associated weight loss, malaise and myalgia.
On examination she was afebrile, very pale and normotensive
(110/60 mmHg). The dorsalis pedis and posterior tibial artery
pulsations were palpable bilaterally and synchronously but the
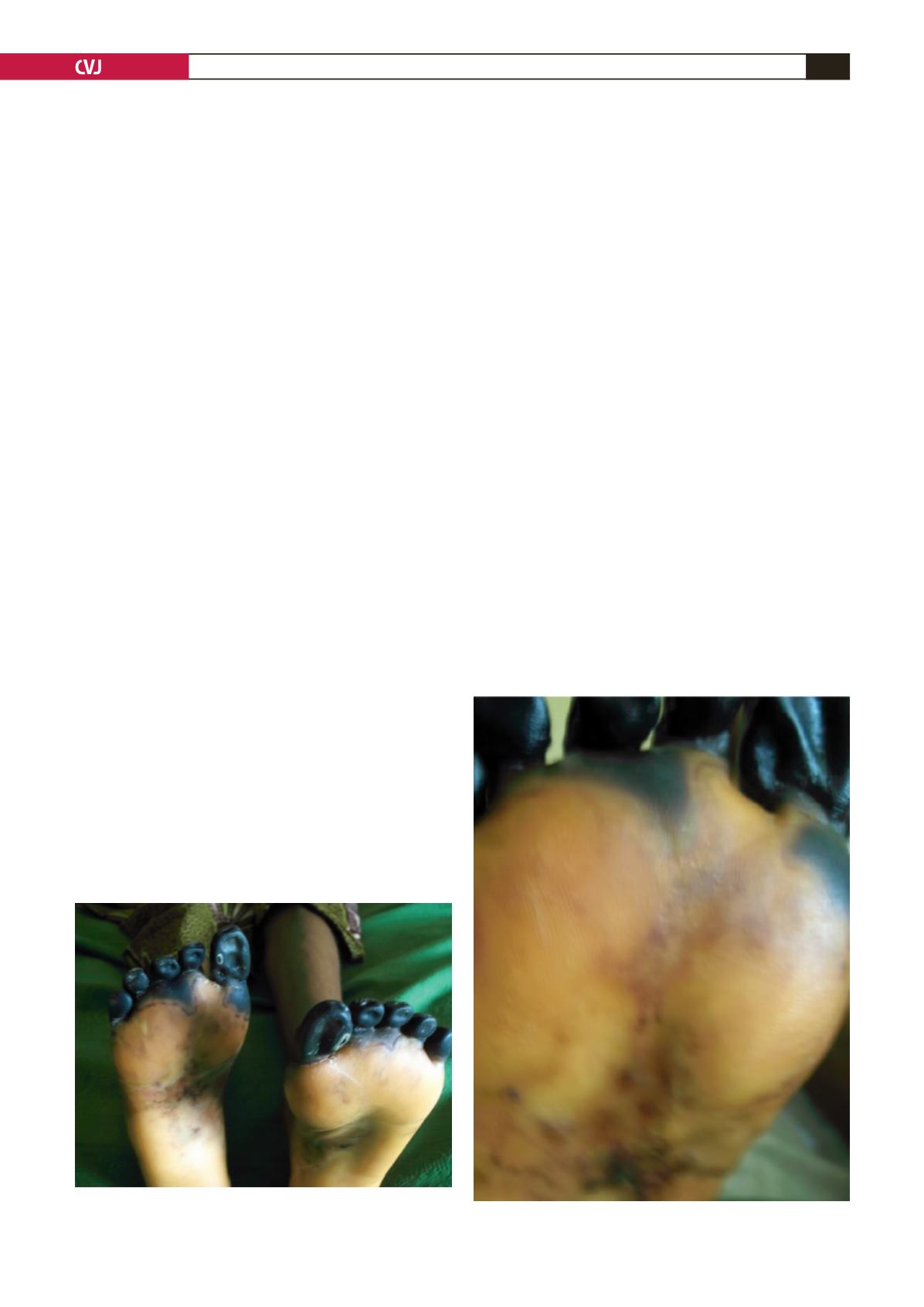
intensity appeared equally reduced on both sides. There was
black discoloration and demarcation of her toes, with a stocking-
pattern loss of sensation and vasculitis on her feet (Figs 1, 2).
The rest of the clinical examination, which included a detailed
assessment of the cardiovascular system, was unremarkable.
Doppler studies showed reduced distal flow in the digital
arteries supplying her toes. Foot radiographs were normal.
An initial working diagnosis of autoimmune vasculitis with
gangrene was made. The differential diagnoses considered were:
systemic lupus erythematosis, antiphospholipid syndrome and
any of the overlap syndromes.
Her laboratory results showed anaemia (haemoglobin 7.8 g/
dl), renal impairment (serum urea 17.7 mmol/l, creatinine 224
µ
mol/l, estimated GFR 42.9 ml/min/1.73m
2
), proteinuria 3
+
,
Fig. 1. Gangrene of the toes in a young Nigerian girl with
antiphospholipid syndrome.
Fig. 2. Vasculitis in the same patient.


