















 62 / 68
62 / 68

CARDIOVASCULAR JOURNAL OF AFRICA • Volume 30, No 3, May/June 2019
e2
AFRICA
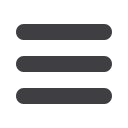
diagonosis of ALCAPA syndrome was made (Fig. 1). The
RCA was dilated and tortuous and there were well-developed
collaterals between the LCA and RCA.
Corrective surgery was planned. Under cardiopulmonary
bypass, the pulmonary artery was resected, the origin of the LCA
was prepared as a button, mobilised 4 cm and implanted directly
onto the left side of the ascending aorta. A graft interposition to
the main pulmonary artery was performed with a 20-mm PTFE
tube. The bypass pump was switched off without any problems.
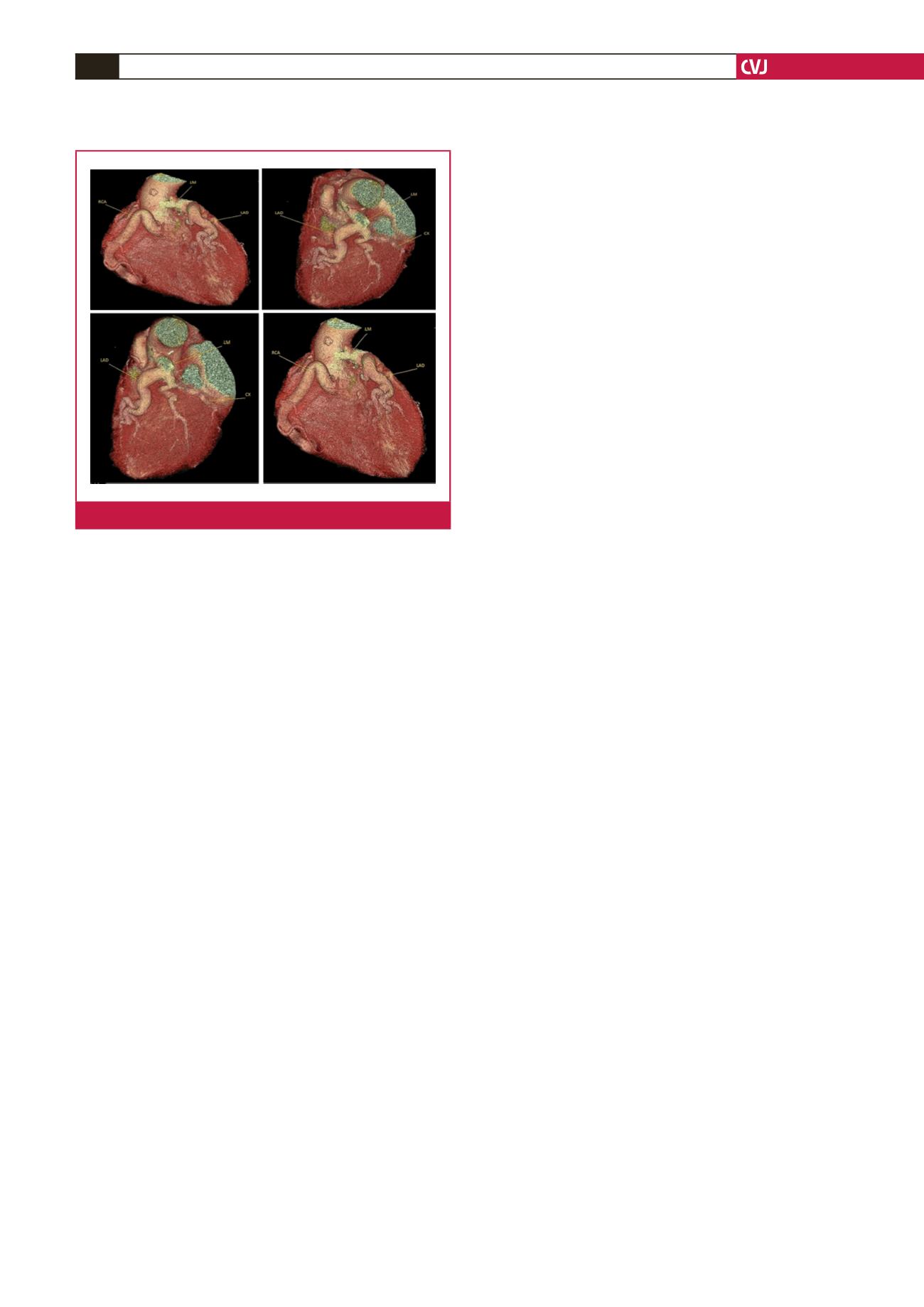
In the control CCTA one week after surgery, the LCA was
noted to be normal (Fig. 2). The patient was discharged on the
10th postoperative day.
Discussion
ALCAPA syndrome is a rare congenital malformation. It occurs
in one out of 300 000 live births and constitutes about 0.25–0.5%
of all congenital heart defects.
1
The major determinants for
symptoms in patients with this condition are the development
of collaterals and myocardial ischaemia. The level of symptoms
due to ischaemia depends on the degree of development of
collaterals between the LCA and RCA.
3
Adult-type ALCAPA includes patients with well-developed
collaterals, while those without collaterals have the infantile type
of this syndrome.
3
Unless this infantile type is diagnosed and
treated, 90% of children die in their first year of life because of
heart failure due to widespread myocardial ischaemia and mitral
regurgitation.
1,4
Adult patients can present with angina, dyspnoea,
syncope, myocardial infarction or arrhythmias. Sudden cardiac
death secondary to malignant ventricular arrhythmias is the
most common presentation.
1,3
The few patients who do survive
to adulthood without surgery have plentiful, well-formed inter-
coronary collaterals with adequate perfusion of the LV.
2
Chattranukulchai
et al
. performed corrective surgery on a
79-year-old female patient, who had been admitted to hospital
with a three-month history of shortness of breath, after
diagnosing her with ALCAPA.
2
The abnormal origin of the
LCA from the pulmonary artery, the left coronary artery flow
via Doppler imaging, the dilated RCA, severe left ventricular
dysfunction and mitral regurgitation can be detected by TTE.
1,4
In our patient, we detected reverse flow in the pulmonary artery
by colour and continuous-wave Doppler on TTE.
CCTA is an important non-invasive diagnostic tool that
can be useful to determine the abnormal origin, projection and
collaterals of the coronary arteries.
1
In our case, we performed
CCTA and detected the abnormal origin of the LCA from the
pulmonary artery and the collaterals between the LCA and RCA.
In adult patients, especially those with symptoms and
large left-to-right shunts, surgical correction is recommended;
however, surgery is also recommended by many authors in
asymptomatic individuals in order to prevent subendocardial
myocardial ischaemia, ventricular arrhythmias and sudden
death.
3
There are several surgical approaches, including single
and double coronary artery repairs.
1
Single coronary artery
repair, performed by ligation of the anomalous LCA at its
pulmonary origin, has been abondoned due to the high rate
of complications, including recanalisation of the ALCAPA,
a greater risk of atherosclerosis, severe mitral regurgitation
resulting from ischaemic cardiomyopathy and persistent risk of
sudden death due to silent ischaemia.
1,3
Double coronary artery repairs are preferred nowadays.
These include coronary button transfer, the Takeuchi procedure,
and placement of a coronary artery bypass graft combined with
ligation of the origin of the LCA.
4
We performed button transfer
of the LCA onto the aorta in our patient.
The degree of collateral development and related LCA
perfusion in ALCAPA syndrome determines the occurence of
symptoms. Since our patient had well-developed collaterals to the
LCA, she was asymptomatic and able to give birth 13 times via
the vaginal route without any problem. We can concluded that
very well developed collaterals that effectively supply the LCA
territory can prevent cardiac dysfunction and symptoms, even in
patients with stressful conditions such as pregancy and delivery.
Conclusion
In patients with an ALCAPA diagnosis, good LCA perfusion,
TTE showing normal left ventricular function, no wall-motion
defects and angiographically good collateral blood flow will hide
the symptoms and cause delayed disgnosis.
References
1.
Turkmen S, Yolcu M, Sertcelik A, Cuce MA, Batyraliev T. Anomalous
origin of the left coronary artery from the pulmonary artery syndrome
in an adult and his eight-year follow-up results.
Turk Gogus Kalp Damar
2014;
22
: 632–635.
2.
Chattranukulchai P, Namchaisiri J, Tumkosit M, Puwanant S,
Vorasettakarnkij Y, Srimahachota S,
et al
. Very late presentation of
anomalous origin of the left coronary artery from the pulmonary artery:
case report.
J Cardiothorac Surg
2018;
13
: 70.
3.
Ozer N, Deniz A, Do
ğ
an R. Left anterior descending coronary artery
originating from the pulmonary artery: a rarity suspected during echo-
cardiography.
Turk Kardiyol Dern Ars
2008;
36
: 181–183.
4.
Esmaeilzadeh M, Hadizadeh N, Noohi F. Anomalous origin of the left
coronary artery from the pulmonary artery (ALCAPA) in an old adult.
J Tehran Heart Cent
2011;
6
: 148–151.
Fig. 2.
Postoperative computed tomography imaging.