















 61 / 68
61 / 68

CARDIOVASCULAR JOURNAL OF AFRICA • Volume 30, No 3, May/June 2019
AFRICA
e1
Case Report
A patient with anomalous origin of the left coronary
artery from the pulmonary artery (ALCAPA syndrome)
and 13 live births
Mustafa Yolcu, Mehmet Salih Bilal, Mustafa Kemal Avsar, Ozgur Yildirim
Abstract
Anomalous origin of the left coronary artery from the pulmo-
nary artery (ALCAPA) or Bland–White–Garland syndrome
is a rarely seen congenital anomaly. Adult and infantile types
are defined according to the degree of collateral development
between the left coronary artery (LCA) and right coronary
artery (RCA). If left untreated, ALCAPA has a 90% mortal-
ity rate in the first year of life, primarily due to myocardial
ischaemia and heart failure. The degree of collateral develop-
ment and the related LCA perfusion in ALCAPA syndrome
determine the occurence of symptoms. Herein, we present
a case of a female patient who had previously, without any
symptoms, given live birth to 13 babies. She had been experi-
encing exertional angina, which started long after the delivery
of her 13th child. Since our patient had well-developed collat-
erals to the LCA, she was asymptomatic and able to give birth
to the children via the vaginal route without any problems.
Having well-formed collateral vessels between the RCA and
LCA may prevent patients from developing symptoms, and
even stressful conditions such as pregnancy may be tolerable.
Keywords:
ALCAPA syndrome, surgical, live birth
Submitted 18/4/18, accepted 15/1/19
Published online 6/2/19
Cardiovasc J Afr
2019;
30
: e1–e2
www.cvja.co.zaDOI: 10.5830/CVJA-2019-003
Anomalous origin of the left coronary artery from the pulmonary
artery (ALCAPA) or Bland–White–Garland syndrome is a
rarely seen congenital anomaly.
1
The major determinants for
symptoms in patients with this condition are the development
of collaterals and myocardial ischaemia.
1
The enlarged, tortuous
right coronary artery (RCA) and its collaterals provide retrograde
flow to supply the left ventricle (LV), then preferentially direct it
into the lower-pressure pulmonary artery.
2
Herein, we present a case of a female patient who had
previously, without any symptoms, given live birth to 13 children.
The patient was treated surgically.
Case report
A 56-year-old female patient was admitted to our clinic with
exertional angina that was relieved at rest. Her past medical
history was normal except for 13 live vaginal deliveries.
Electrocardiography was in sinus rhythm without any
pathological ST-T abnormalities. The physical examination
revealed a 2/6 murmur at the mesocardiac area. Her transthoracic
echocardiography (TTE) was normal without any wall-motion
abnormality and the ejection fraction was within normal limits.
On continuous-wave and colour Doppler echocardiography we
detected reverse flow in the pulmonary artery and mild mitral
regurgitation. In the exercise stress test, a 3–4-mm ST-segment
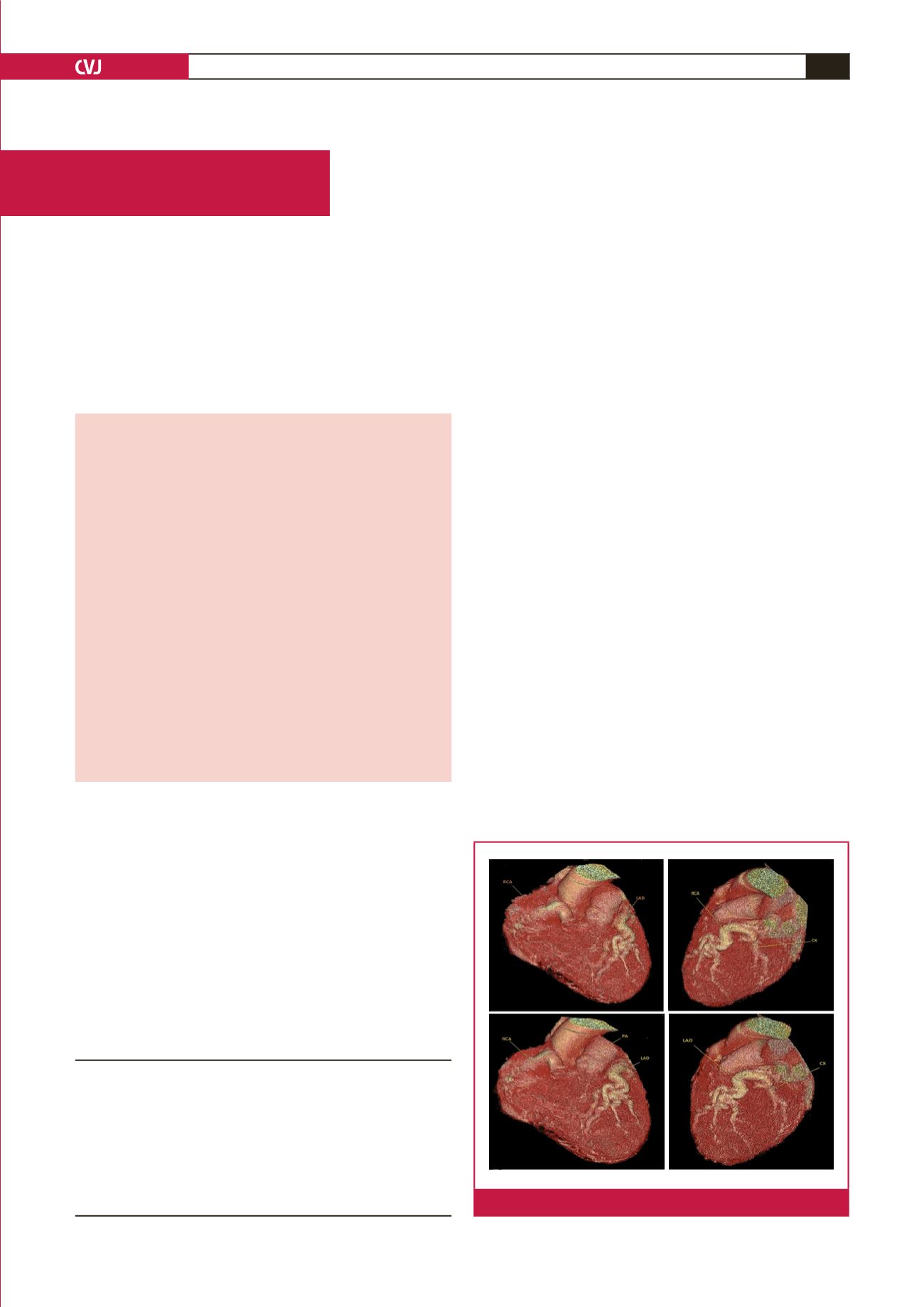
depression was detected in V3 to V6. In coronary computed
tomography angiography (CCTA), the left coronary artery
(LCA) was shown to arise from the pulmonary artery and a
Department of Cardiology, Private Medicana International
Istanbul Hospital, Arel University, Istanbul, Turkey
Mustafa Yolcu, MD,
yolcudoctor@gmail.comDepartment of Cardiovascular Surgery, Private Medicana
International Istanbul Hospital, Istanbul, Turkey
Mehmet Salih Bilal, MD
Mustafa Kemal Avsar, MD
Ozgur Yildirim, MD
Fig. 1.
Pre-operative computed tomography imaging.