


















 10 / 70
10 / 70

CARDIOVASCULAR JOURNAL OF AFRICA • Volume 30, No 5, September/October 2019
252
AFRICA
Thoracic CT scans were used to confirm pericardial thickening
and calcification, and to demonstrate lymph node enlargement.
Tuberculosis (TB) as the cause for constrictive pericarditis
was inferred from a history of previous diagnosis of tuberculosis
(pulmonary or extrapulmonary), or previous treatment for
tuberculosis. Proven tuberculosis was defined by isolation of the
organism or typical histological findings. Patients in whom the
diagnosis of constrictive pericarditis was incorrect were excluded
from the study population.
Informed consent for HIV testing was obtained from all
patients with suspected constriction who were referred to Inkosi
Albert Luthuli Hospital with a view to surgical pericardiectomy.
Relevant data (demographics, HIV status, clinical symptoms,
signs and symptoms, and laboratory, echocardiographic,
radiological and operative data) and follow-up findings were
extracted.
In the subset that underwent pericardiectomy, constrictive
pericarditis was confirmed intra-operatively by identifying
constrictive features with pericardial thickening and fibrosis.
Surgery was performed by median sternotomy without
cardiopulmonary bypass in all but one patient. At operation
the entire ventricular epicardium, apex and diaphragmatic
surface of the heart was freed. The pericardium was removed
anteriorly extending laterally to the phrenic nerves and the
posterior pericardium was left
in situ
after being freed from the
epicardium. Any resection less than this was deemed a partial
pericardiectomy. Immediate peri-operative mortality was defined
as any death occurring during the index hospitalisation.
The study was approved by the Biomedical Research Ethics
Committee of the University of KwaZulu-Natal (BE 324/15).
Statistical analysis
Data were analysed using Stata 13.0 (StataCorp 2013, Stata
Statistical Software: Release 13, College Station, TX: StataCorp
LP). Continuous variables were summarised using mean
and standard deviation or median and interquartile range.
Differences in means of continuous predictors by HIV status
(two groups) were assessed using the student’s
t
-test. If the data
were not normally distributed then the Kruskal–Wallis equality-
of-populations rank test was employed instead. Association
between HIV status and categorised explanatory variables/
risk factors were assessed using a Pearson chi-squared (
χ
2
) test.
Multivariate logistic regression was employed to estimate the
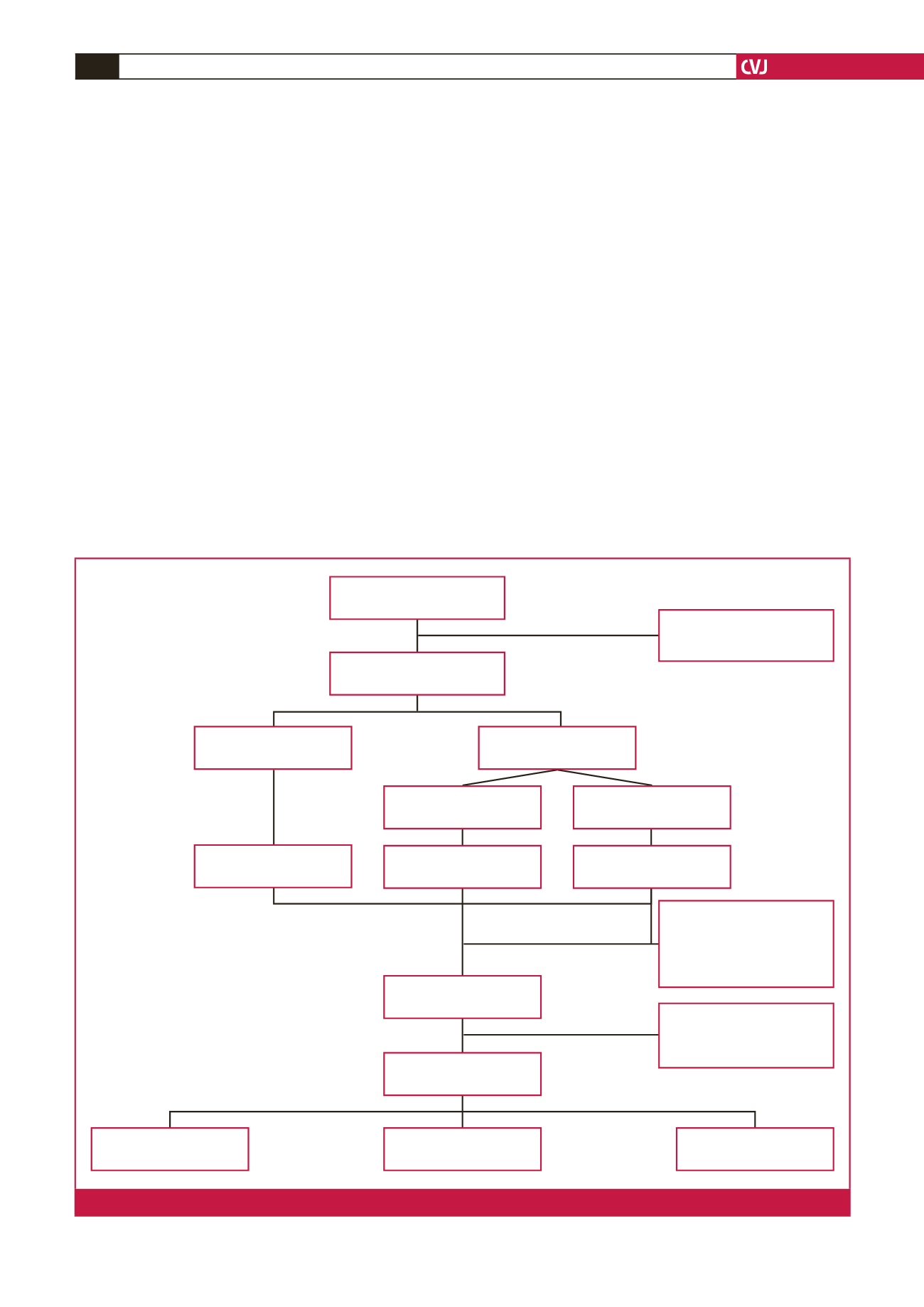
Evaluated for CP
n
=
86
Excluded,
n
=
3
• 2 patients did not have CP
• 1 patient’s HIV status was unknown
Confirmed CP with known HIV status
n
=
83
HIV negative
n
=
51 (62%)
HIV positive
n
=
32 (39%)
Pericardiectomy
n
=
16 (66.7%)
CD4 < 200 cells/mm
3
n
=
8 (15%)
CD4 > 200 cells/mm
3
n
=
24 (75%)
Pericardiectomy
n
=
32 (62%)
Pericardiectomy
n
=
5 (63%)
Did not undergo pericardiectomy
• 14 died pre-operatively
–
–
4 in hospital
–
–
10 out of hospital
• 15 still alive but lost to follow up
• 2 survival status unknown
Not followed up:
• 3 in-hospital peri-operative deaths
• 1 lost to follow up
• 6 referred back to base hospital f/u
Total undergoing pericardiectomy
n
=
52 (63%)
Alive at 6/52 weeks’ follow up
n
=
42
HIV positive CD4 < 200 cells/mm
3
n
=
4 (9.5%)
HIV positive CD4 > 200 cells/mm
3
n
=
12 (29%)
HIV negative
n
=
26 (62%)
Fig. 1.
Early outcome of patients with constrictive pericarditis (CP).