
















 68 / 76
68 / 76

CARDIOVASCULAR JOURNAL OF AFRICA • Volume 29, No 4, July/August 2018
e2
AFRICA
keeping with anaemia of chronic diseases. The prostate-specific
antigen level was mildly elevated. Chest radiography revealed a
mildly increased cardiothoracic ratio and hyperinflated lungs.
Unfortunately, the patient refused further hospital management,
including surgery, and died a year later.
Patient 2: The second patient was a 32-year-old male of Indian
descent who presented with a two-month history of abdominal
pain, weight loss and diarrhoea. He had no significant past
medical, surgical, family or occupational history.
His clinical examination revealed features of right heart
failure with severe tricuspid and moderate pulmonary valve
regurgitation. The rest of his examination was unremarkable.
Chest radiography revealed a mildly increased cardiothoracic
ratio and an electrocardiogram revealed sinus rhythm. Blood
results revealed mild pre-renal dysfunction, anaemia of chronic
disease, normal liver function test and normal comprehensive
metabolic panel. Further biochemical results revealed an elevated
5-HIAA level and prior to referral, his private practitioner had
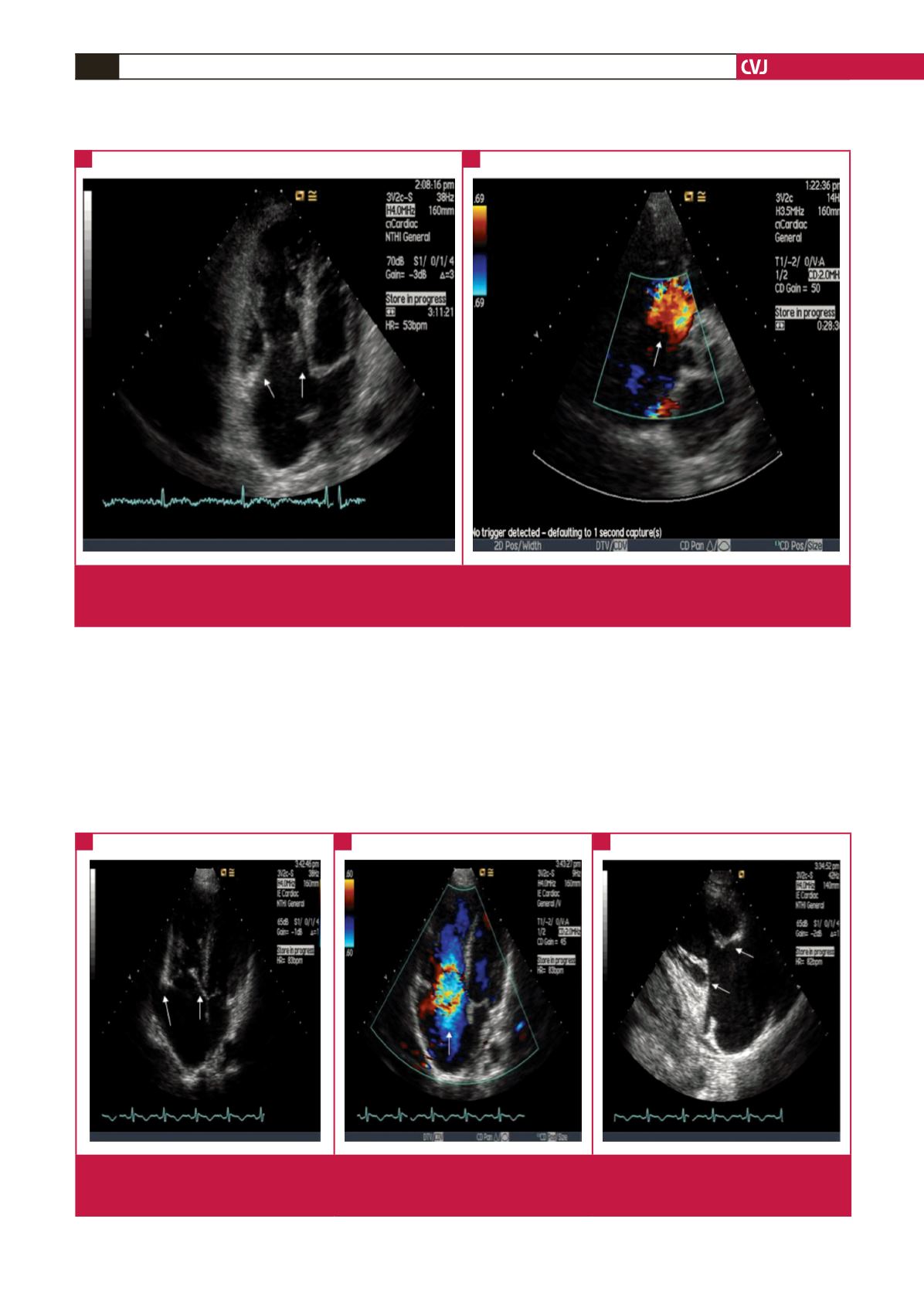
Fig. 1.
Patient 1. (A) Apical four-chamber view showing tricuspid leaflets that are thickened and retracted (arrows). The right ventricle
and atrium are dilated. (B) Colour Doppler with free flow through the tricuspid valve during systole in a parasternal short-axis
view at the level of the aortic valve (arrow).
A
B
Fig. 2.
Patient 2. (A) Apical four-chamber view: note the thickened, immobile and retracted tricuspid leaflets and minimally thickened
mitral valve leaflets (arrows), and the dilated right atrium and ventricle. (B) Torrential tricuspid regurgitation (note the arrow).
(C) Marked failure of coaptation (indicated by arrows) of the tricuspid valve leaflets.
A
B
C