
















 69 / 76
69 / 76

CARDIOVASCULAR JOURNAL OF AFRICA • Volume 29, No 4, July/August 2018
AFRICA
e3
already commenced medical therapy, which included octreotide.
Two weeks later the patient was referred for a specialist’s
opinion and further management. His echocardiographic and
computed tomographic images are presented in Figs 2 and 3,
respectively. His symptoms improved dramatically on medical
therapy and he was subsequently referred to the surgical team,
where an elective tricuspid valve replacement (TVR) was
successfully performed six months later. His intra-operative
and postoperative periods were uneventful, and his symptoms
continued to improve on subsequent follow-up visits.
Discussion
Prevalence of carcinoid syndrome and CHD
Reports have indicated that at least 50% of patients with
clinical manifestations of carcinoid syndrome present with
echocardiographic evidence of cardiac or cardiovascular
involvement.
1-5
At least a quarter of carcinoid patients with
cardiac manifestations present with right-sided cardiac disease.
Although CHD is undoubtedly regarded as a rare entity, it is
an interesting and important cause of intrinsic tricuspid and
pulmonary valve disease and is associated with significantly high
morbidity and mortality rates. Tricuspid and pulmonary valve
regurgitations usually occur as secondary phenomena due to
dilatation of the valve annular ring, secondary to right ventricular
failure or as a result of severe pulmonary hypertension.
Previous reports have indicated that the incidence of carcinoid
tumours occurs at a rate of 1.2 to 2.1 in 100 000 of the general
population.
6,7
In most instances, at the time of diagnosis,
20 to 30% of patients present with carcinoid syndrome and
approximately 50% of these patients develop CHD, which
typically causes abnormalities of the right side of the heart.
5,8,9
In an estimated 20% of patients with carcinoid tumours, CHD is
the primary presentation of the metastatic carcinoid disease.
5,8,9
Although it is usually believed that carcinoid tumours that
have hepatic involvement are highly associated with pathological
cardiovascular damage, particularly right-sided cardiac
involvement related to the large amount of metabolic products
reaching the heart, a small proportion of patients, around five
to 10%, present with significant left-sided disease due to direct
blood flow from the right to the left side of the heart, or in
some cases related to the presence of a primary lung tumour. In
addition, cardiac manifestations of carcinoid syndrome could
also be related to the paraneoplastic effects of vasoactive
substances released by malignant cells rather than any direct
metastatic involvement of the heart. Most importantly, patients
with progressive cardiac disease tend to have higher levels of these
vasoactive substances compared to those without cardiac disease.
Cardiac and cardiovascular structural changes in CHD
Typical pathological features of CHD are plaque-like deposits
of fibrous tissue deposited on the endocardium of the valvular
cusps and leaflets, atria and ventricles, sometimes involving the
downstream aspects of the tricuspid and pulmonary valves,
endocardium of the cardiac chambers, intima of the vanae cavae,
pulmonary artery and coronary sinus (Figs 1, 2).
Although the fibrous tissue may result in distortion of the
valves, the morphology of the valve leaflets is classically not
disrupted. However, the endocardial thickening may lead to
valve retraction and fixation (Figs 1, 2).
The tricuspid valve is most commonly involved, with
typical tricuspid valvular regurgitation and rarely stenosis.
The pulmonary valve is the second most commonly affected,
presenting as mixed pulmonary valve disease. Pulmonary
stenosis is more frequently noted, compared with tricuspid
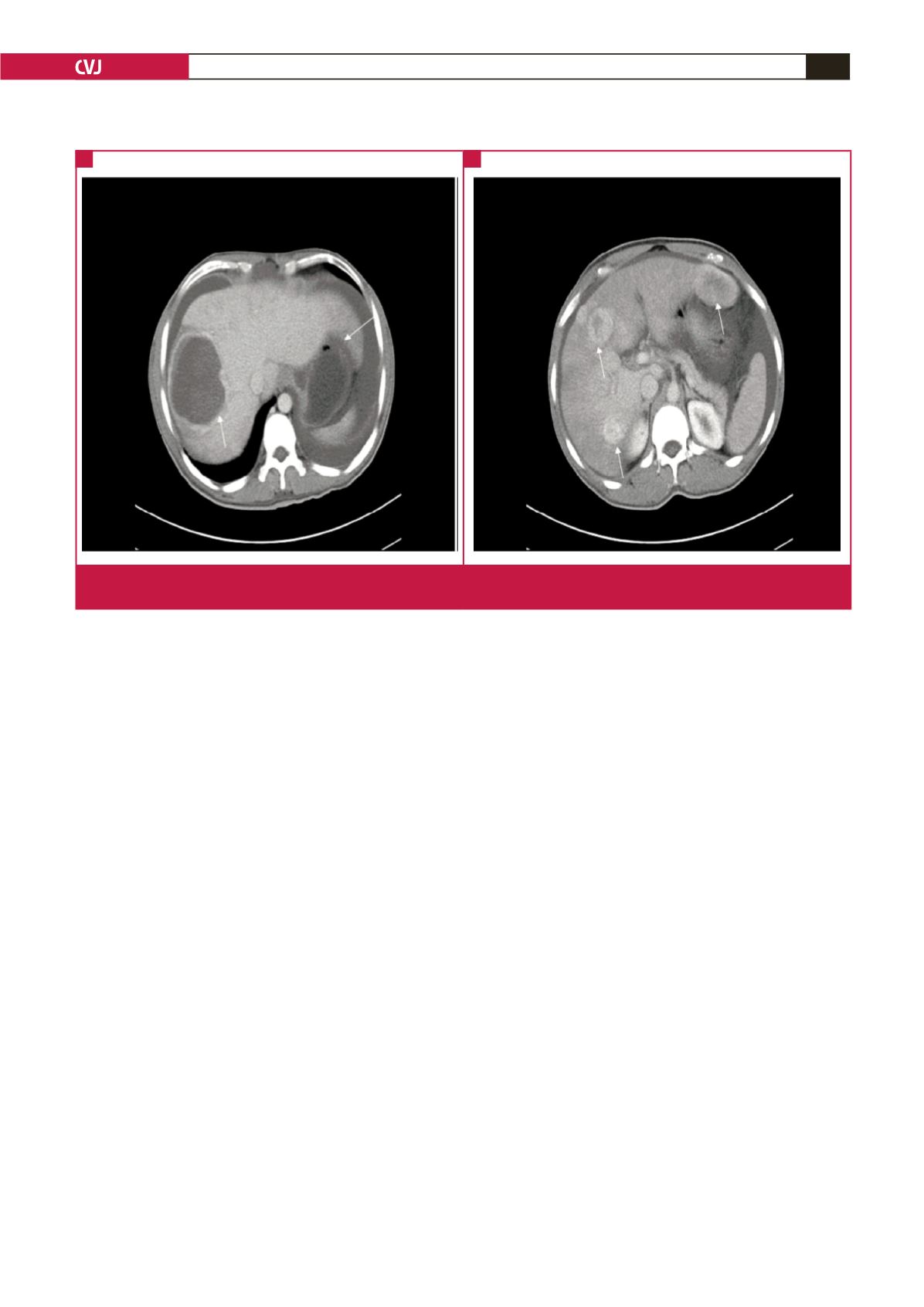
Fig. 3.
Patient 2. Computed tomography scan. Notice a large echogenic mass on the right lobe of the liver, and further multiple
echogenic masses on both lobes (arrows).
A
B