















 57 / 67
57 / 67

CARDIOVASCULAR JOURNAL OF AFRICA • Volume 26, No 2, March/April 2015
AFRICA
e3
Case Report
A case of May–Thurner syndrome with inconsistent
radiological and surgical findings
Fatih Akin, Serhat Aygun, Niyazi Gormus, Yeter Duzenli Kar, Hanife Tugce Susam, Ahmet Ozel
Abstract
May–Thurner syndrome is the result of compression of the
left common iliac vein between the right common iliac artery
and the overlying vertebrae. In this case report, we describe
an 11-year-old boy presenting with swelling of the left lower
extremity. An iliac MR venography showed compression of
the left proximal iliac vein between the vertebra and the left
iliac artery. In surgery, it was seen that the left common iliac
vein was connected to the postero-inferior part of the inferior
vena cava, and it was compressed between the right common
iliac artery and the columna vertebralis, which was inconsist-
ent with the radiological findings. An interposition of the
great saphenous vein graft between the left common iliac
vein and the inferior vena cava was made, with a successful
outcome. Our case is interesting in that it showed inconsistent
findings between the radiological images and surgery.
Keywords:
May–Thurner syndrome, child, leg swelling
Submitted 18/6/13, accepted 27/1/15
Cardiovasc J Afr
2015;
26
: e3–e5
www.cvja.co.zaDOI: 10.5830/CVJA-2015-013
Iliac vein compression syndrome, also known as the May–
Thurner syndrome (MTS), is the result of compression of the
left common iliac vein between the right common iliac artery and
the overlying vertebrae. Although it was first described in 1908
by McMurrich, a detailed anatomical description was generated
by May and Thurner in 1956.
1,2
This compression may cause focal intimal proliferation of the
vein, and subsequently venous stasis of the left lower extremity
occurs. MTS manifests as left lower extremity swelling, pain,
venous stasis changes, and deep venous thrombosis (DVT).
3
The
usual presentation of MTS is compression of the left iliac vein
by the right common iliac artery and the overlying vertebrae.
4
Here we describe a case of MTS whose radiological findings
showed an atypical compression of the left iliac vein by the left
iliac artery.
Case report
An 11-year-old boy presented to our institution with left
lower extremity swelling. The swelling had first appeared two
years earlier and had progressed slowly. The swelling increased
after standing for a long time or walking more than 500 m. It
decreased with overnight rest but did not resolve completely.
Occasionally, he had mild pain in his calf while standing. There
was no history of surgery or a central venous indwelling catheter.
A review of his systems was negative for chest pain, shortness
of breath, cough, fever, malaise, visual changes, headache,
weakness, or pain and swelling in other areas of the body. He
had no significant family history of cancer, blood clots, cardiac
problems, early death or use of antithrombotic agents.
On arrival, his blood pressure was 100/60 mmHg and the
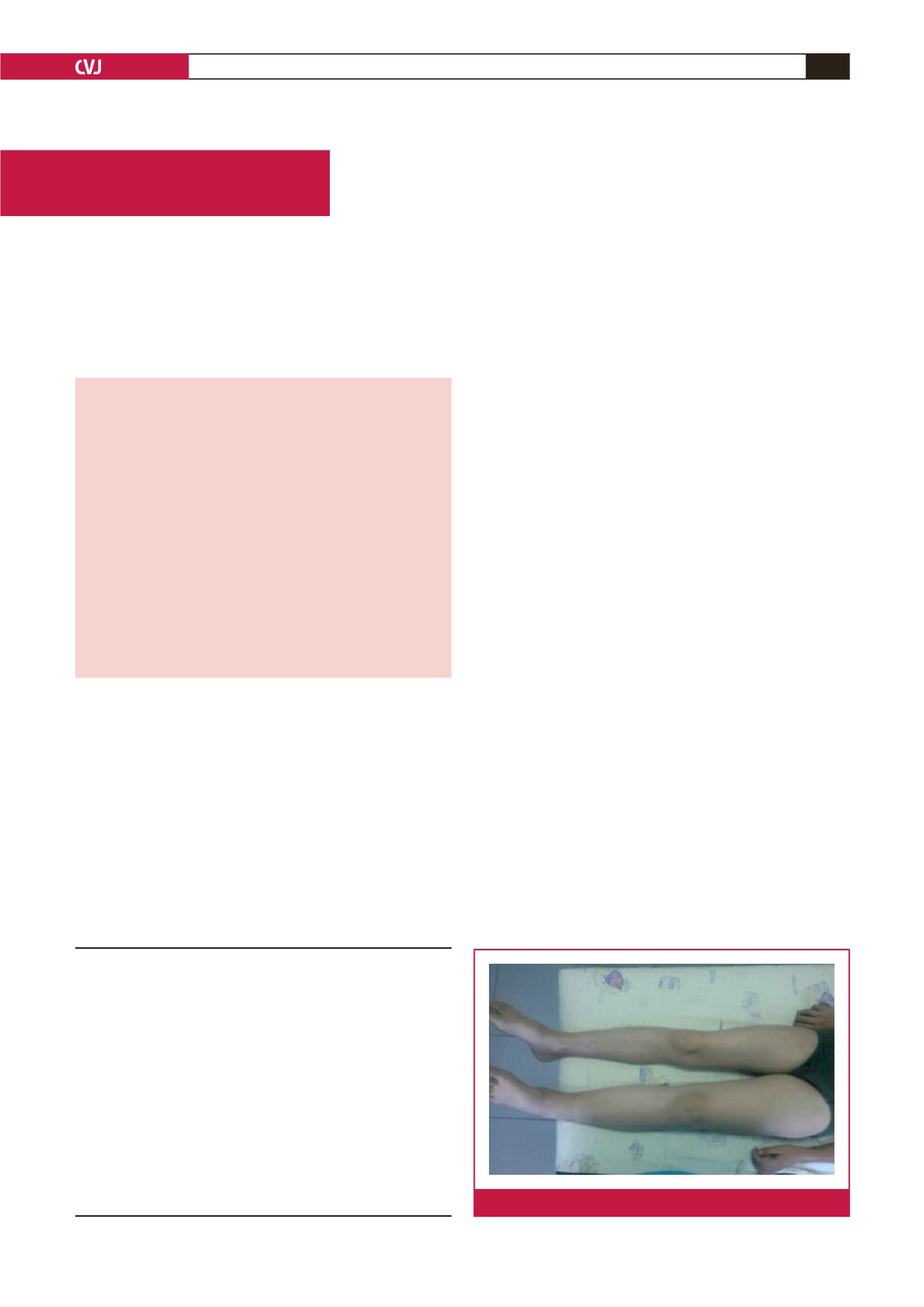
pulse rate was 102 beats/min. On physical examination there was
diffuse swelling of the left lower extremity, starting at the groin
and progressing distally (Fig. 1). The left calf was tense and
Department of Pediatrics, Konya Training and Research
Hospital, Konya, Turkey
Fatih Akin, MD,
drfatihakin@gmail.comYeter Duzenli Kar, MD
Hanife Tugce Susam, MD
Department of Radiology, Konya Training and Research
Hospital, Konya, Turkey
Serhat Aygun, MD
Department of Cardiovascular Surgery, School of
Medicine, Necmettin Erbakan University, Konya, Turkey
Niyazi Gormus, MD
Department of Pediatric Nephrology, Konya Training and
Research Hospital, Konya, Turkey
Ahmet Ozel, MD
Fig. 1.
Swelling of the left lower extremity of the patient.