
















 9 / 68
9 / 68

CARDIOVASCULAR JOURNAL OF AFRICA • Volume 26, No 6, November/December 2015
AFRICA
207
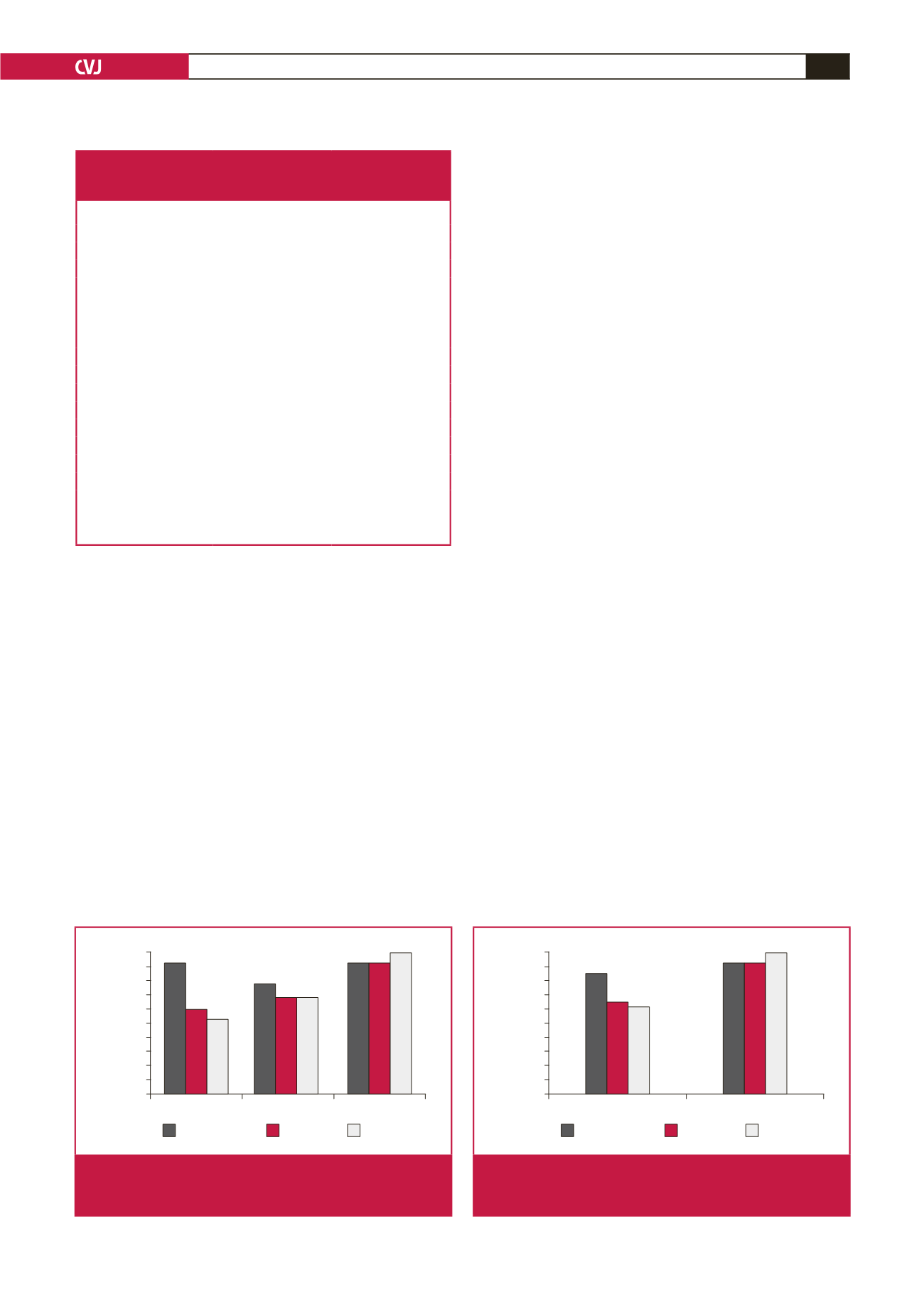
On the other hand, a statistically significant difference was not
detected between H-FABP, TnI and CK-MB levels in the patient
group that was admitted after more than six hours (
n
=
14). Figs
1 and 2 compare the AI values of the cardiac markers according
to admission times after onset of symptoms.
False-negative results were obtained in four patients who
were tested for H-FABP, and false-positive results were obtained
in two. Although all characteristics of these six patients were
reviewed in detail with the hope of finding any predictors for
false negativity and false positivity, no characteristics could be
detected to explain this condition.
Discussion
In our study, the role of bedside H-FABP measurement was
investigated in 48 patients who were admitted to the emergency
room within 12 hours of onset of chest pain lasting for more
than 30 minutes and who did not have ST-segment elevation on
ECG. It was concluded that H-FABP was a better diagnostic
marker than CK-MB and Tn I, with high sensitivity (79%) and
specificity (93%) (AI
=
85%) for early diagnosis of NSTEMI (
≤
six hours). In addition, the sensitivity and specificity of H-FABP
for the group admitted
≤
three hours of onset of symptoms were
calculated as 89 and 100%, respectively.
H-FABP is seen as a novel cardiac marker in the diagnosis
of ACS. Nakata
et al
.
22
and O’Donoghue
et al.
23
have shown it
to be an early diagnostic and prognostic marker. It begins to
elevate in the plasma within one to three hours following the
initial symptoms of ACS and decreases to normal levels within
24 to 36 hours.
10
A few immunohistochemical methods are used for the
detection of H-FABP levels and these take from 45 minutes to
16 hours. This time decreases to 15 minutes with CardioDetect,
a single-step, qualitative bedside test. Values
>
7 mg/l are seen
as positive.
20
In a previous study conducted on 38 patients, this
bedside method was compared with the ELISA method, which is
used for the quantitative measurement of H-FABP levels, and it
was completed in 45 minutes. These two methods were therefore
similarly successful in making a diagnosis.
20,24
Recent studies in the literature on the diagnostic value of
H-FABP in ACS have given controversial results.
25,26
Some
studies showed H-FABP to be a reliable diagnostic tool for the
early diagnosis of ACS/MI,
14-16
and others displayed negative
results.
17-19
In the study by Glatz
et al
.
9
conducted on 83 patients, the
diagnostic sensitivity of H-FABP was shown to be better than
that of myoglobin in patients who were admitted within six
hours of onset of symptoms (78 vs 53%,
p
<
0.05). Similarly,
in the study by Haastrup
et al
.,
27
which was conducted on
130 patients who did not have ST-segment elevation and were
admitted in under six hours, the sensitivity of H-FABP was
found to be 90–95% and specificity was 81–94% for different
reference values. Myoglobin and H-FABP were reported to be
useful markers in the early triage of patients with chest pain.
In the study by Yoshihiko
et al
., which was conducted on
129 patients suspected of AMI, the sensitivity of H-FABP was
found to be 100% and specificity was 63% in the first three
hours.
28
Patients with STEMI were included this study. In the
same study, the sensitivity of troponin T (TnT) was found to
be 50% and specificity was 96% in the first three hours. They
concluded that H-FABP was a more valid marker than TnT in
Table 5. Diagnostic value of H-FABP, TnI and CK-MB in
NSTEMI diagnosis, according to admission time after
onset of symptoms (
≤
6 and
>
6 hours)
≤
6 hours (
n
=
34)
>
6 hours (
n
=
14)
H-FABP
Sensitivity (%)
79
100
Specificity (%)
93
89
NPV (%)
78
100
PPV (%)
94
83
AI (%)
85
93
TnI
Sensitivity (%)
53
100
Specificity (%)
80
89
NPV (%)
57
100
PPV (%)
77
83
AI (%)
65
93
CK-MB mass
Sensitivity (%)
37
100
Specificity (%)
93
100
NPV (%)
54
100
PPV (%)
88
100
AI (%)
62
100
Accuracy index (%)
≤
3 h
3–6 h
>
6 h
100
90
80
70
60
50
40
30
20
10
0
Tnl
H-FABP
CK-MB
p
<
0.01
p
<
0.05
p
>
0.05
Fig. 1.
AI values of H-FABP, TnI, and CK-MB for the diagnosis
of NSTEMI according to admission times (
≤
3, 3–6,
and
>
6 hours).
Accuracy index (%)
≤
6 h
>
6 h
100
90
80
70
60
50
40
30
20
10
0
Tnl
H-FABP
CK-MB
p
<
0.05
p
>
0.05
Fig. 2.
AI values of H-FABP, TnI and CK-MB for the diagnosis
of NSTEMI according to admission times (
≤
6 and
>
6 hours).