















 53 / 64
53 / 64

CARDIOVASCULAR JOURNAL OF AFRICA • Volume 27, No 1, January/February 2016
AFRICA
51
right common iliac artery as the donor vessel. Complex repair
of the right renal artery followed, with subsequent right renal
auto-transplantation onto the iliac vessels. Formal closure of
the abdomen was performed three days later, at which point it
was found that there was minimal thrombus in the abdominal
aneurysm.
The patient subsequently had an uneventful course. His
creatinine level improved to 73
μ
mol/l (MDRD estimated
glomerular filtration rate was 117 ml/min/1.73 m
2
) and his
blood pressure normalised without additional antihypertensive
medication. He was discharged in good health and was attending
the vascular out-patient clinic regularly, with normal renal
function.
Discussion
The condition was first described in South Africa, with the
earliest cases dating back to a publication by Pepler in 1955.
9
The term ‘intimomedial mucoid degeneration’ was first used
in 1977 by Decker
et al
. from Johannesburg in their case series
of nine patients with aortic aneurysms.
1
Due to the lack of
understanding of its aetiology, the condition was defined in
pathological terms describing its histological features.
1,10,11
In 1993 it became apparent that IMMD also had extra-
aortic manifestations, when Cooper
et al.
from Durban
published a series of six cases in which the subclavian,
common carotid, mesenteric and iliac arteries were found to
have IMMD.
11
In our case the right subclavian, left common
carotid, right superficial femoral and left renal arteries were
involved. Recent reports have also shown IMMD to affect
smaller vessels, such as the coronary, brachial, dorsalis pedis
and temporal arteries.
5,7
Although early publications reported IMMD to be confined
to predominantly female black South Africans, subsequent
publications from India and Europe demonstrated that the
disease is not limited to the African population.
4,8,12
This is
illustrated in our case as our patient was of mixed ancestry
and male. Various studies have shown that aneurysms in
IMMD affect a younger population group than what is found
in conventional non-specific degenerative aneurysms.
1,4,6
As
in this case, patients with IMMD have a high prevalence of
hypertension, which aggravates the elastic tissue breakdown,
resulting in aneurysm formation.
1,4,6,9,11
Patients with IMMD present with localised symptoms related
to the position of the aneurysms.
7,9
Presenting symptoms include
abdominal and back pain, presence of a pulsatile mass, limb
claudication and symptoms related to aneurysm rupture.
6
This
could be explained by the most common sites of involvement
being the infra-renal aorta, followed by the thoracic aorta,
subclavian, common carotid and common iliac arteries.
6
Our
patient did not present with abdominal or back pain, however,
his chest discomfort could be explained by the local effects of the
aneurysmal descending thoracic aorta.
The morphological characteristics of the aneurysms found
in patients with IMMD are usually of the fusiform or saccular
types.
8
Various imaging modalities, namely duplex ultrasound,
CTA and/or magnetic resonance angiography, are used to
determine the extent of disease, and whether or not there is an
element of dissection.
6,8
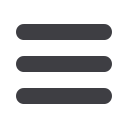
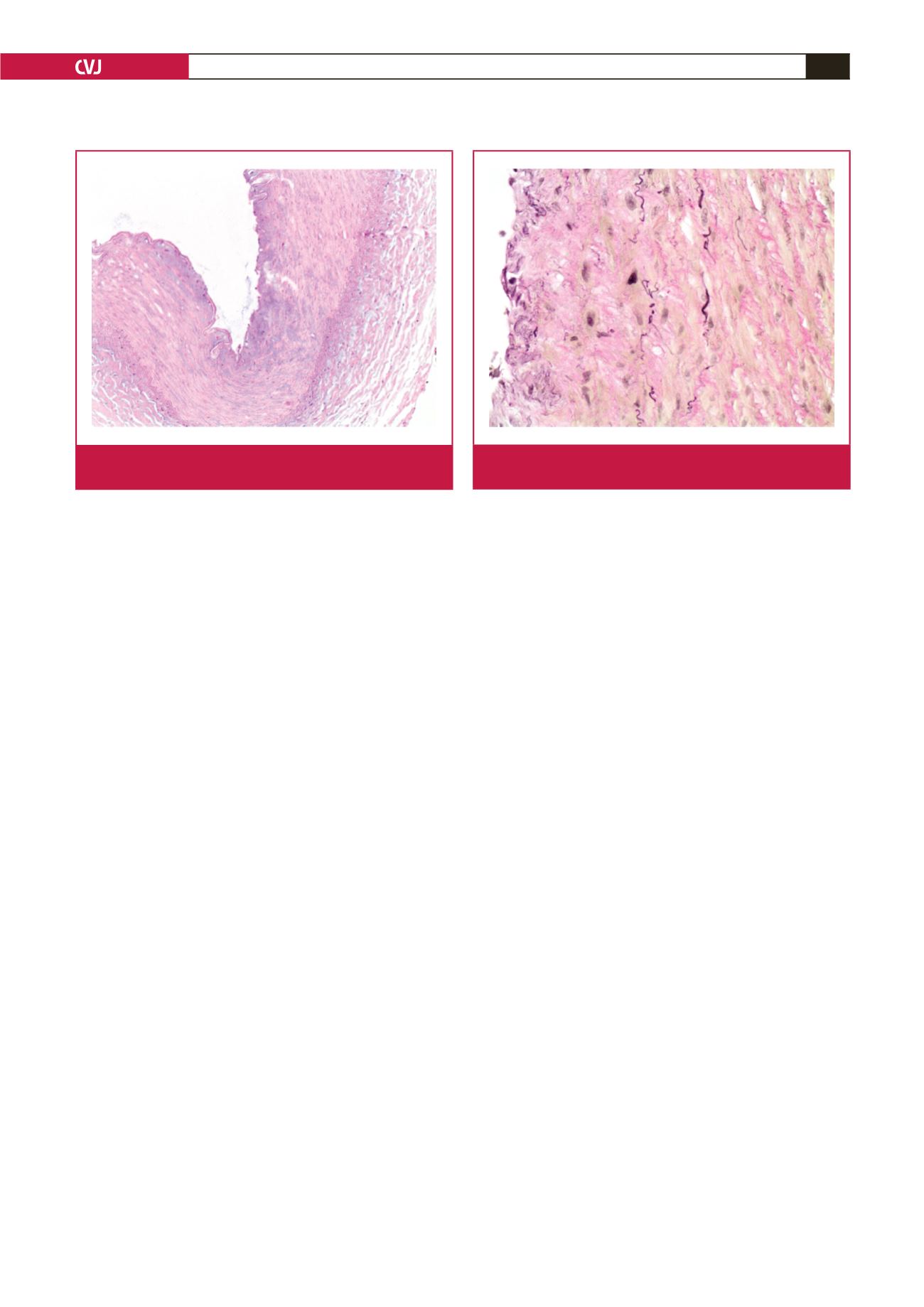
The principle histological features of IMMD include intimal
and medial thickening resulting from accumulation of mucin
pools, which in turn leads to fragmentation and aggregation of
elastin fibres, as illustrated by our case.
8,11
The weakened wall
structure finally results in aneurysm formation.
2,11
A striking
feature on histological examination is the absence of any
inflammatory reaction.
1
The features are distinct from cystic
medial necrosis, in which only the media is affected by the mucin
accumulation.
1,4
Cystic medial necrosis is also typically confined
to the aorta, whereas IMMD has been found to involve extra-
aortic vessels.
1,11
Extra-aortic disease in IMMD may also be
found without any aortic involvement.
2,11
A distinctive feature of IMMD is the paucity of luminal
thrombus in the aneurysm sac.
7
Patients often suffer from
bleeding intra-operatively.
8
This bleeding diathesis is aggravated
by surgical manipulation and is reversed once the aneurysm
is repaired. It is therefore postulated that there is a primary
fibrinolytic process that originates from the diseased aneurysm,
which might explain why a thrombus is seldom found in IMMD,
as was the case in our patient, and why occlusive disease is a rare
finding, apart from a few reports in the literature.
4-6,8
Fig. 5.
Mucin pools within the intima and medial muscle layer
are highlighted on Alcian blue stain (200
×
magnification).
Fig. 6.
The Elastic von Gieson stain highlights fragmentation
of the elastic fibres (400
×
magnification).