















 55 / 64
55 / 64

CARDIOVASCULAR JOURNAL OF AFRICA • Volume 27, No 1, January/February 2016
AFRICA
53
First reported cases: renal denervation with second-
generation multi-electrode catheter via brachial and
radial access
MJ Heradien, J Augustyn, A Saaiman, PA Brink
Abstract
Renal denervation is a minimally invasive procedure that aims
to reduce brain–kidney sympathetic cross-talk. Despite the
negative results of the recent SYMPLICITY HTN-3 trial,
the procedure is considered safe and has been associated with
many beneficial effects, including the reversal of hypertensive
heart disease substrate and the prevention of cardiac arrhyth-
mia. The first-generation radiofrequency catheter system
featured a monopolar catheter that required sequential single-
point energy application, followed by rotation, partial with-
drawal of the catheter and re-application of energy. The
latest generation device features four electrodes configured in
a helical arrangement that can simultaneously ablate in four
quadrants of the vessel circumference. Renal denervation via
brachial or radial arterial access with the second-generation
system has not been described before.
Keywords:
hypertension, renal denervation, atrial fibrillation
Submitted 1/10/15, accepted 14/11/15
Cardiovasc J Afr
2016;
27
: 53–55
www.cvja.co.zaDOI: 10.5830/CVJA-2015-089
Renal denervation (RD) is a minimally invasive procedure that
aims to reduce brain–kidney sympathetic cross‐talk. Despite the
negative results of the recent SYMPLICITY HTN‐3 trial,
1
the
procedure is considered safe and has been associated with many
beneficial effects, including the reversal of hypertensive heart
disease substrate and the prevention of cardiac arrhythmia.
2
The first-generation radiofrequency (RF) catheter system
featured a monopolar catheter that required sequential
single-point energy application, followed by rotation, partial
withdrawal of the catheter and re‐application of energy. The
latest generation device features four electrodes configured in
a helical arrangement that can simultaneously ablate in four
quadrants of the vessel circumference (Fig. 1A). Although
the system is designed for femoral access, brachial or radial
procedural access has possible advantages, including reduced
risk of bleeding and easier access to the renal arteries due to
the acute take-off angles of the renal artery from the abdominal
aorta.
As part of our ongoing trial aiming to determine whether
sympathetic modulation with RD can prevent recurrence
of atrial fibrillation (‘RDPAF’; clinicaltrials.gov identifier:
NCT01990911), we report on two cases of RD with the next
generation RD catheter system performed via brachial or radial
access. The trial was approved by our local ethics committee,
conformed to the Declaration of Helsinki, and the subjects
provided written informed consent.
Case 1: renal denervation via brachial arterial
access
Our first case was a 62-year-old female patient (body mass index
>
30 kg/m
2
) with a history of uncontrolled hypertension and type
2 diabetes mellitus, and paroxysmal atrial fibrillation managed
with rivaroxaban, which was discontinued four days prior to the
procedure. Baseline office blood pressure was 150/90 mmHg.
Routine femoral access was achieved. However, catheter access
to the right renal artery failed due to the acute anatomical take-
off of the vessel. Therefore, it was decided to attempt access via
a brachial approach as an alternative. Percutaneous left brachial
arterial access was achieved with a 6-Fr introducer sheath
(Terumo), 6-Fr multipurpose guiding catheter (Medtronic) and
a 190-cm, 0.014-inch gage BMW
TM
guide wire (Abbott Vascular).
A Symplicity Spyral
TM
(Medtronic) catheter was then introduced
over the guidewire, after removing the straightening tool,
resulting in approximately 125 cm of catheter length (Fig. 1B).
The diameter of the main renal artery was approximately 6.5
and 5.5 mm on the left and right side, respectively. Access to both
arteries was readily attained, and 17 and 13 lesions were created
in the right and left renal arteries, respectively (Fig. 2).
Department of Internal Medicine, Stellenbosch University,
South Africa
MJ Heradien, MB ChB, BSc Hons, MMed (Cert Cardiol)
PA Brink, MB ChB, MMed, PhD
SA Endovascular, Netcare Kuilsriver Hospital, Cape Town,
South Africa
MJ Heradien, MB ChB, BSc Hons, MMed (Cert Cardiol)
J Augustyn, MB ChB, MMed
A Saaiman, MB ChB, MMed
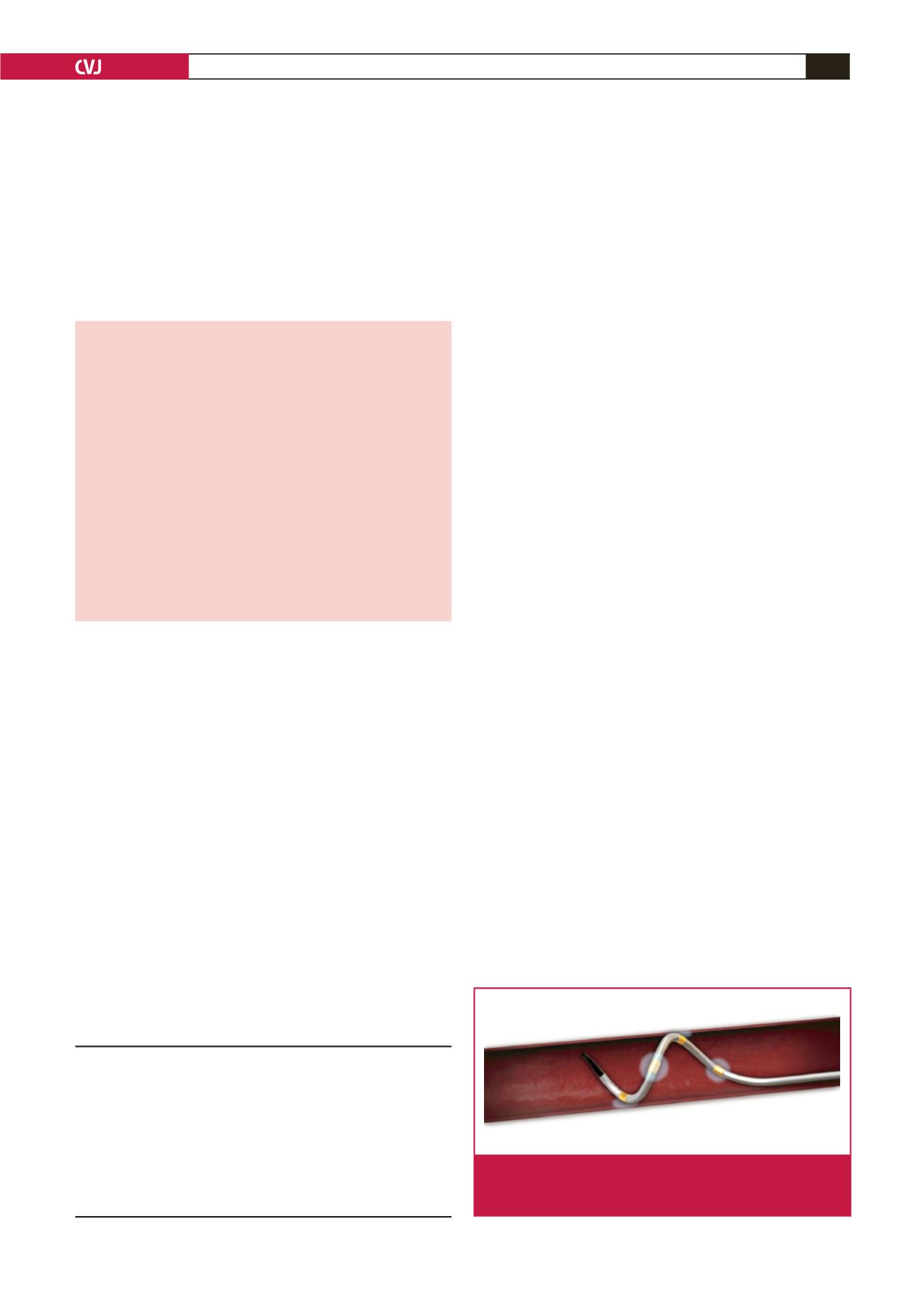
Fig. 1A.
Symplicity Spyral
®
renal ablation catheter is an over‐
the‐wire system that enables simultaneous quadripo-
lar renal artery ablation.