CARDIOVASCULAR JOURNAL OF AFRICA • Vol 23, No 3, April 2012
e2
AFRICA
effusion was most likely due to the scleroderma. We postulated
that after pericardiocentesis, the tract created by the needle
remained open for a period of time due to the nature of the skin
and subcutaneous tissue as a result of her scleroderma. Also
a flap valve was created transiently by her being in the anti-
Trendelenburg position.
Discussion
Hydropneumopericardium is a rare condition which usually
arises from a fistula created between the pericardium and the
oesophagus, or a diaphragmatic hernia, and in one instance
a pancreatic pseudocyst.
1,2
This can also arise after trauma or
following surgery.
Spontaneous
hydropneumopericardium
following
unsuccessful percutaneous pericardiocentesis for a post-
cardiac surgical pericardial effusion has been noted, as well as
following serofibrinous pericarditis, and also in a patient with
endomyocardial fibrosis.
3,4
Due to the underlying cause being
a fistula, most patients require surgical drainage to prevent
tamponade and to address the underlying cause.
5
Surgery is
usually performed as an emergency procedure and the mortality
rate of this condition has been reported to be as high as 58%.
Conclusion
This case illustrates the classic echo features of hydro-
pneumopericardium in the context of an unusual clinical
scenario and is to our knowledge the first documented case of
spontaneous resolution. It also highlights documented serious
complications of percutaneous pericardiocentesis, a procedure
that is not without problems.
References
1.
Vidi V, Singh PP, Alhumaid AC, Lee RS, Kinnunen PM.
Hydropneumopericardium. Presenting as an acute coronary syndrome:
a rare complication of paraesophageal hernia
. Tex Heart Inst J
2009;
36
(3): 255–258.
2.
Hardikar JV, Mistry RC, Patel CV. Hydropneumopericardium due to
ruptured traumatic pseudocyst of pancreas (a case report).
J Postgrad
Med
1986;
32
(4): 241–242.
3.
Wu M, He X, Yang G. Spontaneous tension hydropneumopericardium
complicating serofibrinous pericrditis.
Eur J Cardiothorac Surg
2006;
29
(3): 422–424.
4.
Aidal E, Valori A, Abbruzzenese PA. Postoperative hydropneumoperi-
cardium.
Heart
2004;
90
(9): 1058.
5.
Cummings RG, Wesly RL, Adams DH, Lowe JE. Pneumopericardium
resulting in cardiac tamponade.
Ann Thorac Surg
1984;
37
(6): 511–518.
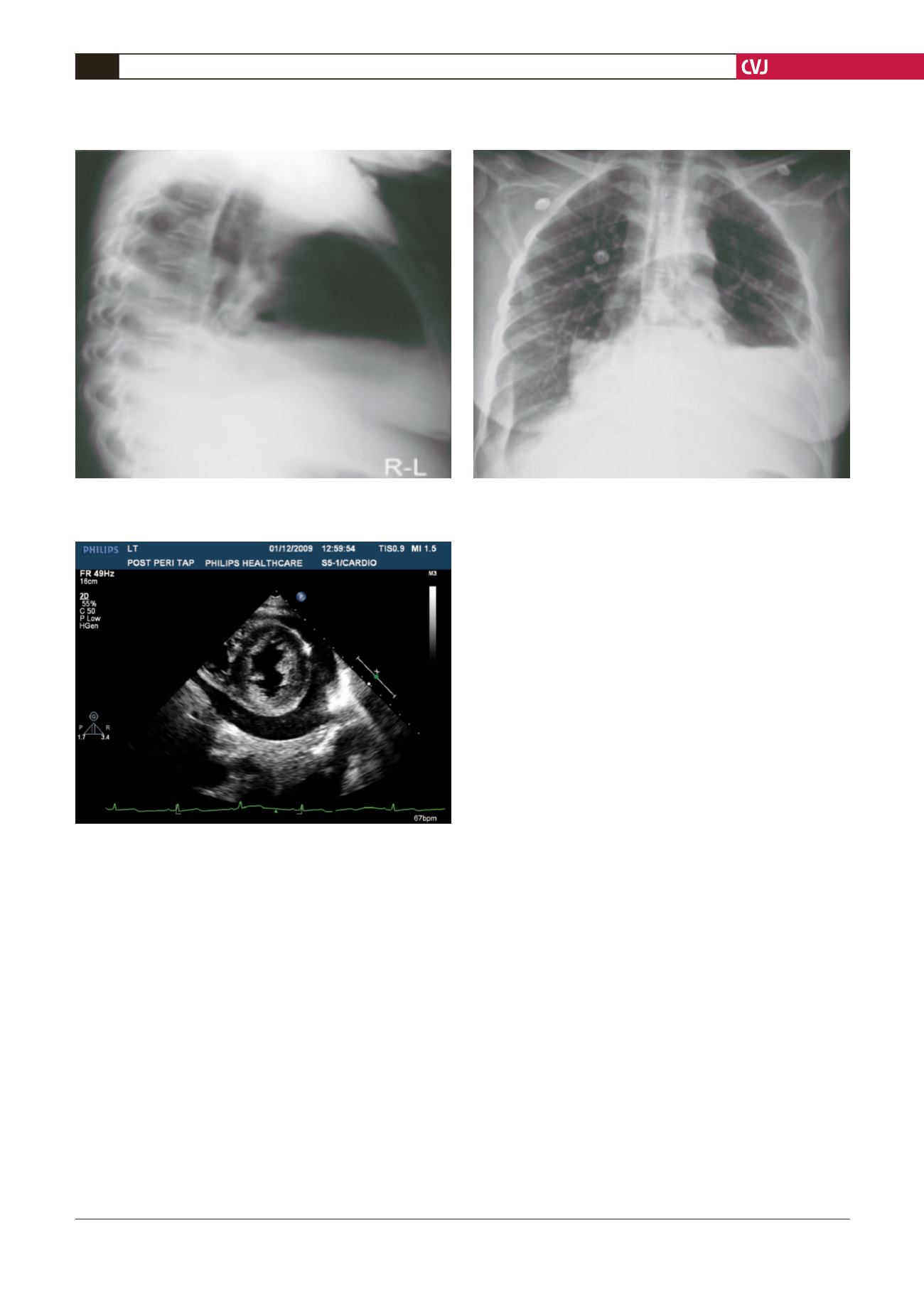
Fig. 4. Parasternal short-axis view demonstrating the
large pericardial effusion with only a few air bubbles left
four days later.
Fig. 3. Chest X-ray demonstrating the air–fluid level, confirming the hydropneumopericardium on both the antero-
posterior and lateral projections.


