CARDIOVASCULAR JOURNAL OF AFRICA • Vol 23, No 6, July 2012
AFRICA
e13
Upon stabilisation of the patient’s general condition,
percutaneous stent implantation was scheduled. Vascular access
was gained by placing 6F sheats in the right femoral and brachial
arteries. Aortic coarctation was crossed retrogrately with a
0.032-inch, 260-cm-long guidewire through a 6F multipurpose
catheter, which was withdrawn and exchanged with a long 12F
sheath (Cook Europe, Bjaeverskov, Denmark). A 45-mm-long
CP stent (Numed Inc, Hopkinton, NY, USA) manually mounted
in a 24 × 40-mm BIB balloon (Numed Inc, Hopkinton, NY,
USA) was then introduced through a long sheath and succesfully
deployed with angiographic control through the right subclavian
artery (Fig. 2).
Post-prosedural angiography confirmed that the stent
placement was adequate and that anatomical results were
excellent (Fig. 3). The patient was discharged free of symptoms
on the second post-procedural day.
At the six-month follow-up examination, the patient was
completely asymptomatic. Echocardiography showed a normal-
sized left ventricle (LVEDD: 55 mm, LVESD: 39 mm) with
normal systolic function (EF: 56%) (Videos 3, 4).
His blood pressure was 130/80 mmHg. Control of his
hypertension was achived with an angiotensin converting enzyme
inhibitor and low-dose thiazide diuretic combination.
Discussion
Aortic coarctation is the fifth most common congenital
heart disease and accounts for 5 to 8% of all congenital
cardiac anomalies.
3
Heart failure is one of the most frequent
complications and cause of death in the natural history of
aortic coarctation.
4
Aortic coarctation should be considered in
the differential diagnosis of cardiomyopathy in adults.
Similar to aortic stenosis, long-standing afterload excess
in the setting of coarctation may be the mechanism of the
failing heart. In patients with aortic stenosis and severe
heart failure, favourable effects on left ventricular function
have been demonstrated following the relief of afterload
excess by aortic valve replacement.
5
Likewise, improvements
may be expected in patients with aortic coarctation and
cardiomyopathy following surgical or percutaneus correction.
While surgical series of coarctation repair include adult
patients with heart failure, no objective data on pre- and
postoperative left ventricular systolic function are included.
6
A few case reports have been published in the literature
demonstrating some degree of improvement in clinical
and echocardiographic parameters following the relief of
coarctation.
1,7,8
However, it is not known whether correction of
coarctation would reverse all indices of heart failure, in other
words ‘cure heart failure’.
Conclusion
We belive that our experience is unique and shows complete
normalisation of left ventricular size and function with full
functional recovery following correction of coarctation with
stent implantation.
References
1.
Pauly DF, Morss SE, Tanio JW, Irani K, Cameron DE, Schulman SP,
Hare JM. Reduced left ventricular dimension and normalized atrial
natriuretic hormone level after repair of aortic coarctation in an adult.
Clin Cardiol.
1999;
22
(3): 233–235.
2.
Morgan DJ, Hall RJ. Occult aortic stenosis as cause of intractable heart
failure
. Br Med J
1979;
1
: 784–787.
3.
Cetta F, Lichtenberg RC, Clark SE. Adults with congenital heart
disease.
Comprehensive Ther
1992;
18
(2): 33–37
4.
Campbell M. Natural history of coarctation of the aorta.
Br Heart J
1970;
32
(5): 633–640.
5.
Connolly HM, Oh JK, Schaff HV, Roger VL, Osborn SL, Hodge DO,
Tajik AJ. Severe aortic stenosis with low transvalvular gradient and
severe left ventricular dysfunction: result of aortic valve replacement in
52 patients.
Circulation
2000;
101
(16): 1940–1946.
6.
Brouwer RM, Erasmus ME, Ebels T, Eijgelaar A. Influence of age on
survival, late hypertension, and recoarctation in elective aortic coarcta-
tion repair. Including long-term results after elective aortic coarctation
repair with a follow-up from 25 to 44 years.
J Thorac Cardiovasc Surg
1994;
108
(3): 525–531.
7.
Alcibar J, Peña N, Oñate A, Gochi R, Barrenechea JI. Stent implanta-
tion in an adult with coarctation of the aorta in the presence of advanced
secondary heart failure.
Tex Heart Inst J
1999;
26
(2): 143–147.
8.
KimW, Jeong MH, ShimWH, AhnYK, Kang JC. A successful stenting
of the coarctation of aorta in a patient presented with acute pulmonary
edema.
Int J Cardiol
2006;
113
(2): 267–269.
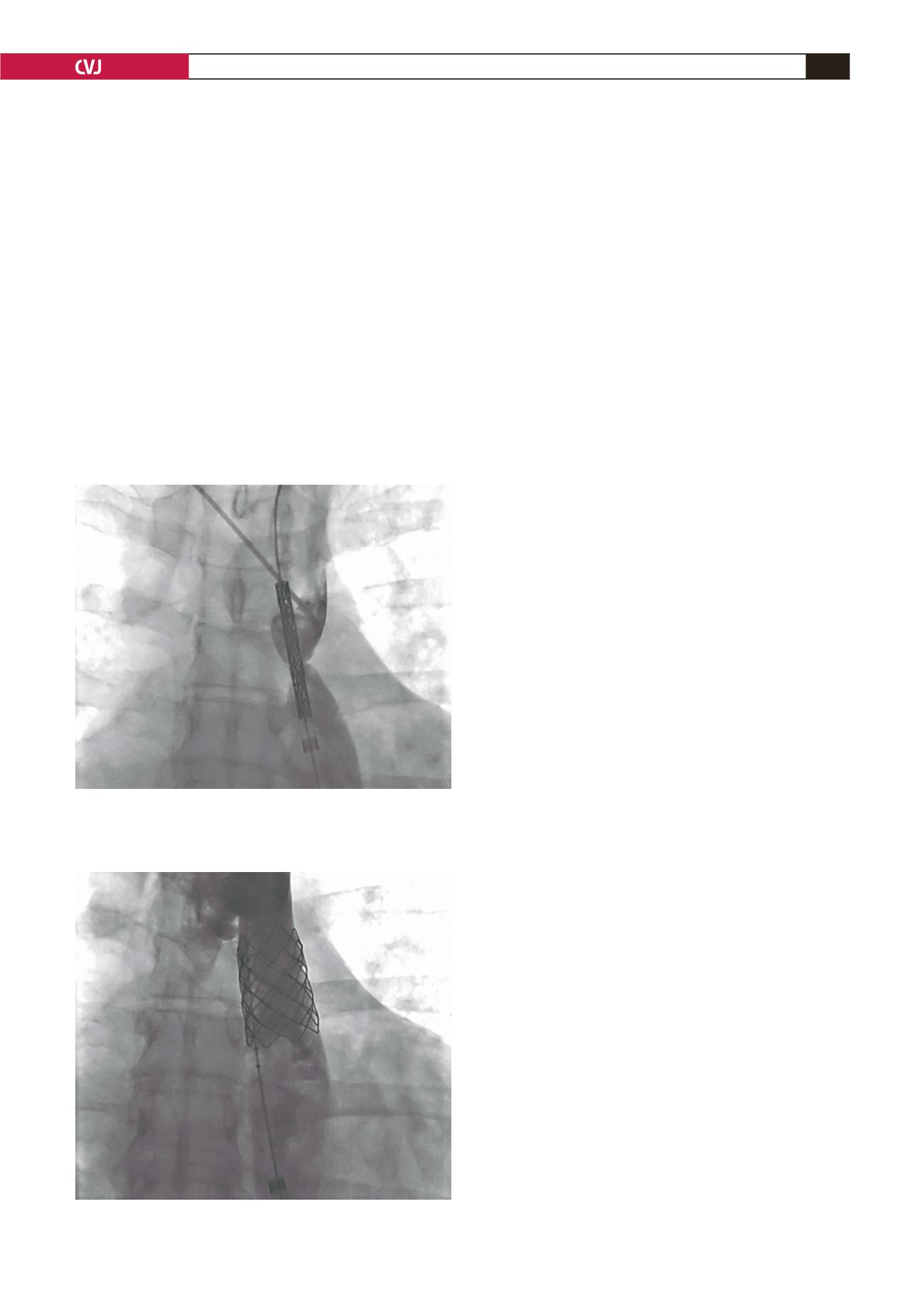
Fig. 2. Introduction of a CP stent mounted in a BIB
balloon under angiographic guidence. Contrast was
administered through a catheter in the right subclavian
artery.
Fig. 3. Angiography following stent deployment.


