CARDIOVASCULAR JOURNAL OF AFRICA • Vol 23, No 6, July 2012
e20
AFRICA
Discussion
LEOPARD is an acronym for the major features of this
rare, dominant, autosomal genetic disease, including multiple
Lentigines (appearing at four to five years and increasing in the
thousands until puberty, independent of sun exposure), ECG
conduction abnormalities, Ocular hypertelorism, Pulmonary
stenosis, Abnormal genitalia, Retardation of growth, and
sensorineural Deafness. As shown here, the diagnosis of LS is
based on multiple lentigines with two or more cardinal features.
1
In the absence of lentigines, three or more other features in
the patient and the presence of an affected close relative are
diagnostic.
The coexistence of lentigines and cardiac disease was first
reported by Walter
et al.
2
in 1966. The defect associated with
development of the syndrome has been located on chromosome
12 and the responsible gene is protein tyrosine phosphatase
non-receptor 11 (PTPN 11). LS is one of the so called
neuro-cardio-facial-cutaneous syndromes, such as Noonan
syndrome, neurofibromatosis type 1, Costello syndrome and
cardiofaciocutaneous syndrome. These overlapping disorders
may represent a differential diagnosis in less complete forms
than reported here. ECG abnormalities occur in about 75% of
the patients, including left, right or bi-ventricular hypertrophy, Q
waves, prolonged QTc and repolarisation abnormalities.
3
Pulmonary stenosis (valvular dysplasia, pulmonary annulus
dysplasia and/or infundibular stenosis) is noted in 20% of
persons with LS. A pre-operative image of the nature of the right
ventricular outflow tract obstruction will determine the form
of operative procedure adopted. Valvulectomy, valvulotomy or
valvuloplasty are possible options.
1
Infundibular and valvular stenosis are common but supra-
valvular stenosis, as reported here, appears to be unusual. Mitral
or aortic valvular anomalies, obstruction of the left ventricular
outflow tract and dilatation of the coronary arteries have seldom
been described in LS and were not observed here.
Right ventricular hypertrophy may also accompany left
ventricular hypertrophy and pulmonary stenosis in about 30%
of patients with LS.
4
Hypertrophic cardiomyopathy (HCM) may
appear later in life and may be life threatening. Careful follow
up of young patients is necessary to detect cardiac conduction
abnormalities (25% of the patients) and the onset of HCM.
Conclusion
LS is probably underdiagnosed. Approximately 200 cases have
been reported in the world and very few in Africa.
1,5
To the best
of our knowledge, this is the first case reported in the horn of
Africa.
References
1.
Sarkozy A, Digilio MC, Dallapiccola B. Leopard syndrome.
Orphanet
J Rare Dis
2008;
27
: 1750–1772.
2.
Walter RJ, Polanski BJ, Grots IA. Electrocardiographic abnormalities in
a family with generalized lentigo.
N Engl J Med
1966;
275
: 1220–1225.
3.
Limongelli G, Pacileo G, Marino B,
et al
. Prevalence and clinical
significance of cardiovascular abnormalities in patients with the
LEOPARD syndrome.
Am J Cardiol
2007;
100
: 736–741.
4.
Limongelli G, Sarkozy A, Pacileo G,
et al
. Genotype-phenotype analy-
sis and natural history of left ventricular hypertrophy in LEOPARD
syndrome.
Am J Med Genet
2008;
46
: 620–628.
5.
Kubeyinje EP, Onunu AN, Obasohan AO. Multiple lentigines syndrome
in a Nigerian family.
Trop Geogr Med
1993;
45
: 135–137.
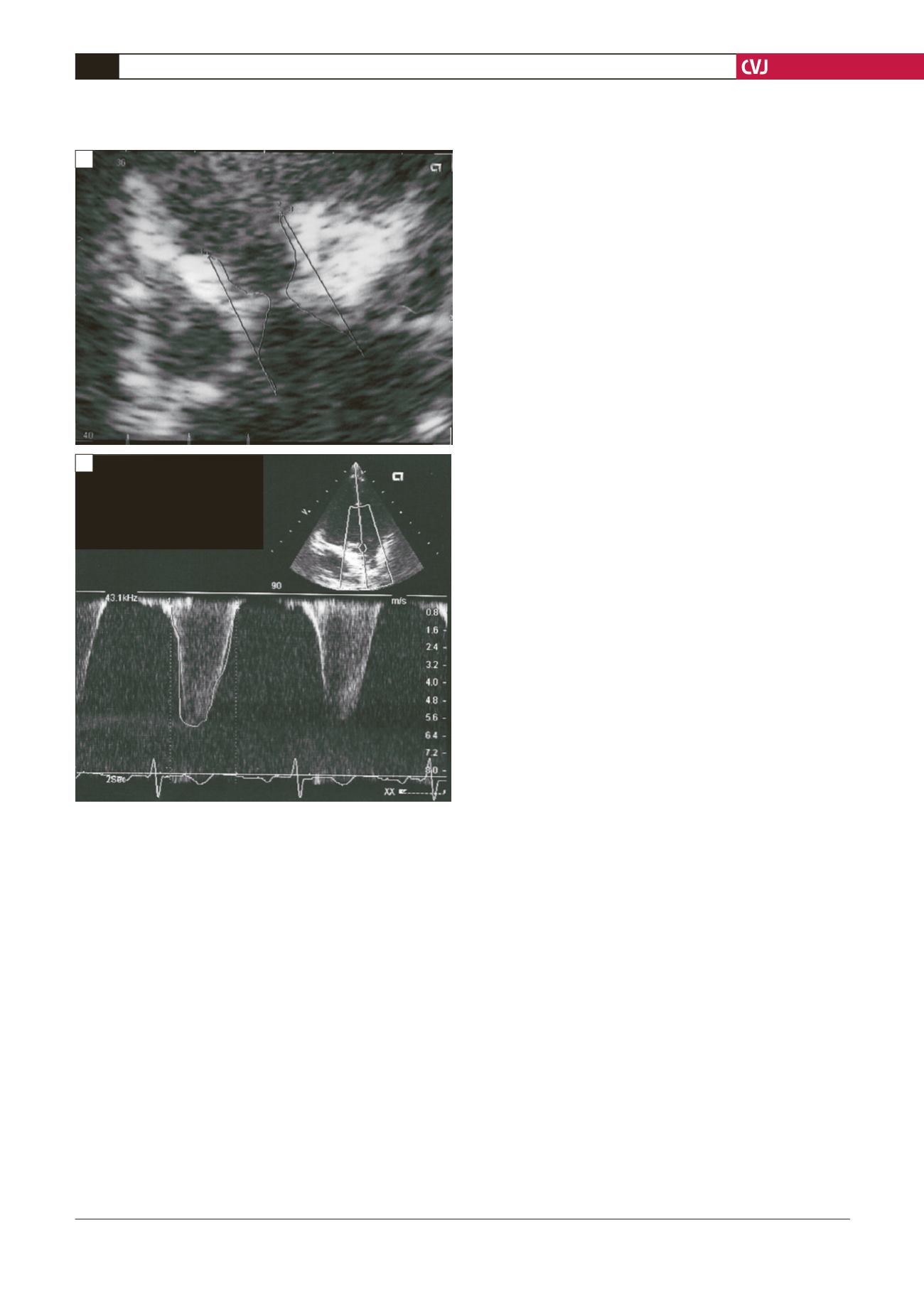
Vmax VP 6.09m/s
VP GPmax 148.5mmHg
VP Vmoy 4.28m/s
VP GPmoy 4.28m/s
ITV VP 154.1cm
HR 75bpm
Right Ventricle
RVOT
Pulmonary
Trunk
Fig. 2. A: Two-dimensional echocardiography of the right
ventricular outflow tract (RVOT), pulmonary annulus
and pulmonary trunk showing a fibrotic stenosis (later
confirmed at surgery). B: Severe pulmonary stenosis
revealed by continuous Doppler: a 148-mmHg peak pres-
sure gradient was measured between the right ventricle
and the pulmonary trunk.
A
B


