CARDIOVASCULAR JOURNAL OF AFRICA • Vol 23, No 6, July 2012
e18
AFRICA
the annulus (89%).
Lack of positive QRS polarities in the inferior leads, positive
QRS polarity in lead aVL, and a greater Q-wave ratio in leads
aVR to aVL were surface ECG characteristics of VT/PVCs
originating from the annulus, which were significantly different
from those of VT/PVCs originating from RVOT. Both right and
left ventricles were activated almost simultaneously, as the origin
of the VT/PVCs was the septum, which caused early precordial
transition on the surface ECG.
2
The QRS morphology in our patient was similar to those
reported by Tada
et al
.
2
for posterior tricuspid annular VT/PVCs.
In their series, among the 38 VT/PVCs originating from the
annulus, three originated from the posterior septum. However, in
contrast to our case, these patients did not demonstrate sustained
VTs but only isolated PVCs from the region of the tricuspid
annulus.
2
Tada and co-workers reported that 66% were treated with RF
catheter ablation. The success rates of RF catheter ablation for
VT/PVCs originating from the free-wall portion of the annulus
and septum were 90 and 57%, respectively.
1
We therefore treated
our case with RF catheter ablation.
Arrhythmias originating anywhere in the right ventricle raise
concerns about the presence of arrhythmogenic right ventricular
cardiomyopathy (ARVC). We performed a cardiac magnetic
resonance imaging study, which revealed a structurally normal
heart in our patient. While ARVC could not be completely
excluded, our case was much more likely to be one of idiopathic
tachycardia, based on the observations of a normal-sized right
ventricle, lack of epsilon waves or inverted T waves in the
precordial leads, absence of fractionated electrograms at or
around the ablation site, suppression of arrhythmia during
exercise, single QRS morphology of the arrhythmia, and the
success of focal ablation.
3
Other than one minor ARVC criterion,
our patient did not fulfil any of the major ARVC criteria, which
also supported the diagnosis of idiopathic VT.
Conclusion
We present a sporadic case of sustained idiopathic VT originating
from the posteroseptal tricuspid annulus. Surface ECG is a
reliable tool that can be used to localise the anatomical origin of
the VT/PVCs.
References
1.
Sergio L. Pinski. The Right Ventricular Tachycardias.
J Electrocardiol
2000;
33
: 103–114.
2.
Tada H, Tadokoro K, Ito S, Naito S, Hashimato T, Kaseno K, Miyaji K,
et al
. Idiopathic ventricular arrhythmias originating from the tricuspid
annulus: prevalence, electrocardiographic characteristics, and results of
radiofrequency catheter ablation.
Heart Rhythm
2007;
4
: 7–16.
3.
O’Donnell D, Cox D, Bourke J, Mitchell L, Furniss S. Clinical and
electrophysiological 7575 differences between patients with arrhythmo-
genic right ventricular dysplasia and right ventricular outflow tract
tachycardia.
Eur Heart J
2003;
24
: 801–810.
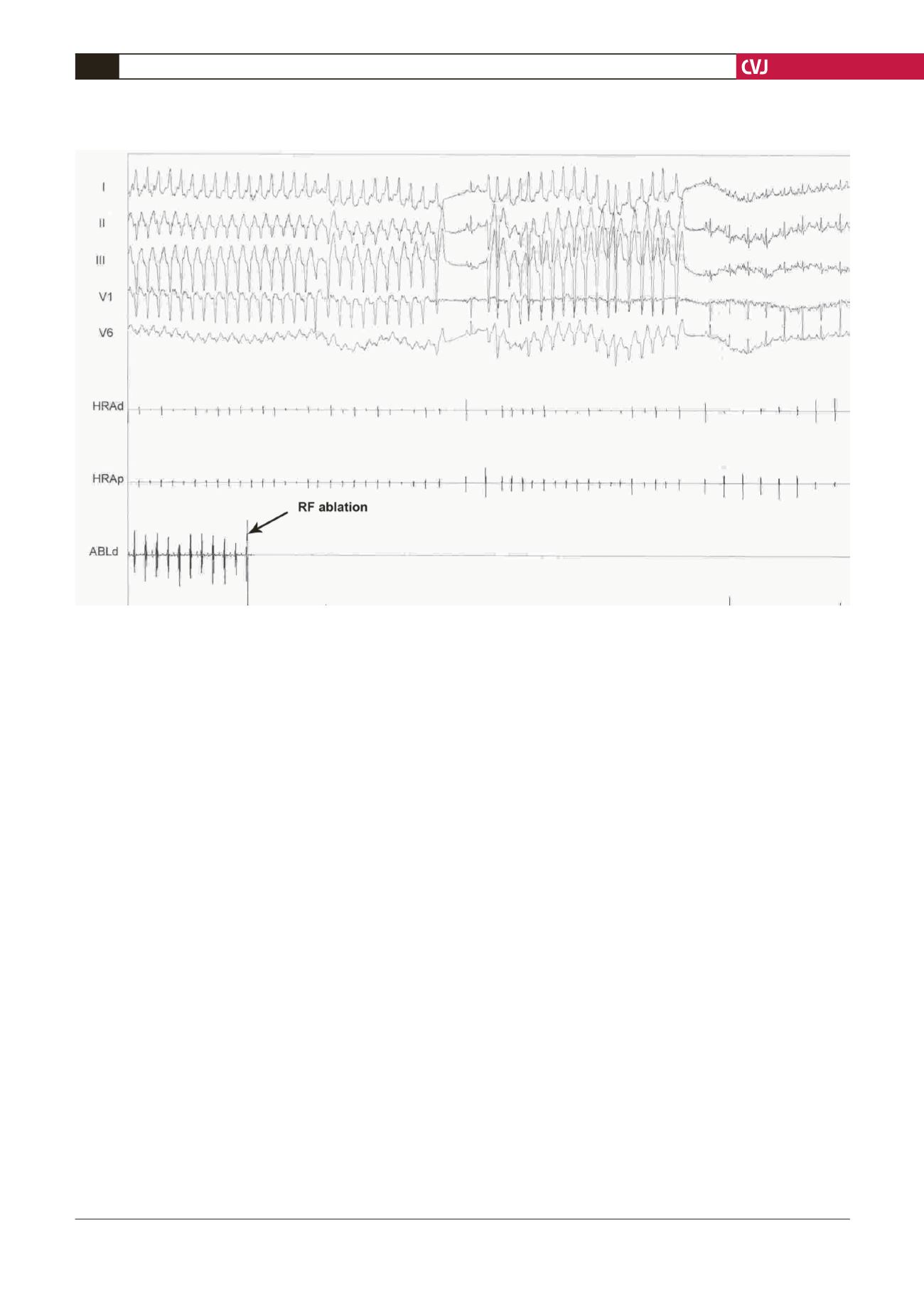
Fig. 3. Intracardiac recordings. After RF energy applications, the tachycardia completely disappeared.


