CARDIOVASCULAR JOURNAL OF AFRICA • Vol 23, No 6, July 2012
AFRICA
e19
Case Report
LEOPARD syndrome
PL MASSOURE, C LATREMOUILLE, G LAMBLIN, F LECA
Abstract
LEOPARD syndrome (LS) is a rare hereditary disorder,
characterised mainly by skin, facial and cardiac abnormali-
ties. We report on the case of a six-year-old Djiboutian with
typical features of LS. Multiple cardiovascular problems are
described, including pulmonary infundibular, valvular and
supra-valvular stenosis. A favourable course was observed
after successful cardiac surgery. This is the first reported
case of LS from the horn of Africa.
Keywords:
LEOPARD syndrome, pulmonary stenosis, ventricu-
lar hypertrophy
Submitted 21/8/10, accepted 22/2/12
Cardiovasc J Afr
2012;
23
: e19–e20
DOI: 10.5830/CVJA-2012-011
LEOPARD syndrome (LS), a rare syndrome comprising
multiple congenital anomalies of the skin, face and heart, is
probably underdiagnosed in Africa. Characteristic cardiovascular
anomalies range from benign to life threatening. We report on
the case of a six-year-old Djiboutian who presented with typical
features of LS.
Case report
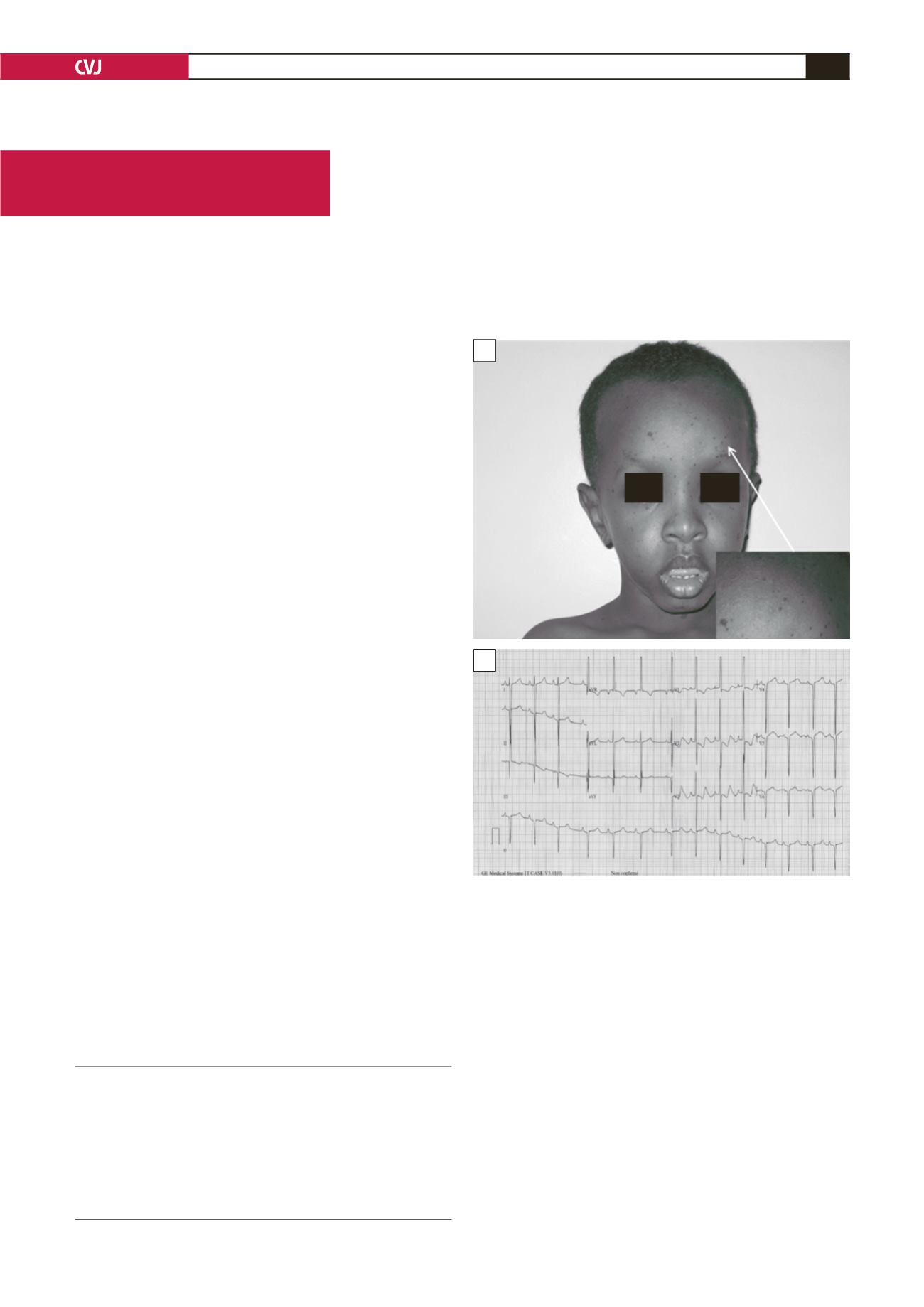
A six-year-old Djiboutian presented with progressive exercise
dyspnoea and flat black-brown lentigines on the face, neck and
torso (Fig. 1A). Physical examination revealed height and weight
below the third percentile, ocular hypertelorism and bilateral
cryptorchism. A grade 3/6 systolic murmur was heard at the left
second intercostal space.
An ECG showed normal sinus rhythm (Fig. 1B) with right
ventricular hypertrophy and long QTc (480 ms). Transthoracic
echocardiography confirmed right ventricular hypertrophy,
especially of the septum and free right ventricular wall, and
revealed pulmonary infundibular, annular and supravalvular
stenosis (Fig. 2A). Peak pressure gradient between the right
ventricle and the pulmonary trunk was 148 mmHg (Fig. 2B).
There was no other cardiac abnormality.
LEOPARD syndrome was diagnosed. There was no other case
in his family. Genetic analyses were not performed.
Surgical procedure consisted of a resection of the fibrotic
stenosis in the right ventricular outflow tract, and widening of
the pulmonary annulus and the first centimetre of the pulmonary
trunk with a pericardial patch. A postoperative echocardiogram
showed a residual 24-mmHg pressure gradient between the right
ventricle and the pulmonary trunk.
After three months of follow up, the patient was asymptomatic.
Conduction abnormalities or rhythm disturbance were not shown
on consecutive postoperative ECG recordings.
Orchidopexy and protection from the sun’s ultraviolet A and
B rays were recommended. The patient’s parent were advised to
avoid drugs known to prolong the QT interval.
Service de Médecine, Hôpital Bouffard, Djibouti, Armées
PL MASSOURE, MD,
G LAMBLIN, MD
Hôpital Européen Georges Pompidou, Paris, France
C LATREMOUILLE, MD
Mécénat Chirurgie Cardiaque – Enfants du Monde, Paris,
France
F LECA, MD
Fig. 1. A: Six-year-old Djiboutian with multiple lentigines
on the face, neck and torso. B: ECG of the patient: sinus
rhythm, deep Q waves, right ventricular hypertrophy and
repolarisation abnormalities (long QTc: 480 ms).
A
B


